
Khác biệt giữa bản sửa đổi của “Amphetamin”
Đã cứu 2 nguồn và đánh dấu 0 nguồn là hỏng.) #IABot (v2.0.8.9 |
Không có tóm lược sửa đổi Thẻ: Thêm thẻ nowiki Trình soạn thảo mã nguồn 2017 |
||
| Dòng 1: | Dòng 1: | ||
{{Drugbox |
|||
| Verifiedfields = changed |
|||
| Watchedfields = changed |
|||
| verifiedrevid = 398687910 |
|||
| IUPAC_name = 1-phenylpropan-2-amine |
|||
| image = Amphetamine-2D-skeletal.svg |
|||
| image2 = Amphetamine-3d-CPK.png |
|||
| imagename = 1: 1 mixture (racemate) |
|||
| drug_name = Amphetamine |
|||
{{Infobox drug |
|||
<!--Clinical data--> |
|||
| IUPAC_name =<div class="center">(''RS'')-1-phenylpropan-2-amine</div> |
|||
| tradename = Adderall |
|||
| image = Amfetamin.svg |
|||
| Drugs.com = {{drugs.com|monograph|adderall}} |
|||
| |
| width = 250px |
||
| alt = An image of the amphetamine compound |
|||
| image2 = D-Amphetamine molecule ball from xtal.png |
|||
| width2 = 250px |
|||
<!-- Clinical data -->| alt2 = A 3d image of the D-amphetamine compound |
|||
| pronounce = {{IPAc-en|audio=En-us-amphetamine.ogg|æ|m|ˈ|f|ɛ|t|ə|m|iː|n}} |
|||
| tradename = Evekeo, [[Adderall]],{{#tag:ref|Adderall and other mixed amphetamine salts products such as Mydayis are not [[Racemic mixture|racemic]] amphetamine - they are a mixture composed of equal parts racemate and [[dextroamphetamine]].<br /> |
|||
''See [[Mixed amphetamine salts]] for more information about the mixture, and [[#Pharmaceutical products|this section]] for information about the various mixtures of amphetamine [[enantiomer]]s currently marketed.''|name=AdderallDiff|group=note}} [[#Pharmaceutical products|others]] |
|||
| Drugs.com = {{Drugs.com|monograph|amphetamine-sulfate}} |
|||
| MedlinePlus = a616004 |
|||
| licence_US =<!--Amphetamine--> |
|||
| DailyMedID = Amphetamine |
|||
| legal_AU = Schedule 8 |
| legal_AU = Schedule 8 |
||
| legal_CA = Schedule I |
| legal_CA = Schedule I |
||
| legal_DE = Anlage III |
|||
| legal_NZ = Class B |
|||
| legal_UK = Class B |
| legal_UK = Class B |
||
| legal_US = Schedule II |
| legal_US = Schedule II |
||
| legal_UN = Psychotropic Schedule II |
|||
| legal_status = Rx-only |
|||
| legal_status =<!--Pharmacokinetic data--> |
|||
| routes_of_administration = [[Mouth|Oral]], [[intravenous]], [[vaporization]], [[Insufflation (medicine)|insufflation]], [[rectal]], [[sublingual]] |
|||
| dependency_liability = Moderate<ref name="Stahl's Essential Psychopharmacology" /> |
|||
| addiction_liability = Moderate |
|||
| routes_of_administration = Medical: [[Oral route|oral]], [[intravenous]]<ref name="Amph Uses" /><br />Recreational: [[Oral route|oral]], [[Insufflation (medicine)|insufflation]], [[Suppository|rectal]], [[intravenous]], [[intramuscular administration|intramuscular]] |
|||
| bioavailability = Oral: {{nowrap|75–100%}}<ref name="Drugbank-dexamph" /> |
|||
| protein_bound = {{nowrap|20%}}<ref name="Drugbank-amph" /> |
|||
| metabolism = [[CYP2D6]],<ref name="FDA Pharmacokinetics" /> [[Dopamine β-hydroxylase|DBH]],<ref name="Substituted amphetamines, FMO, and DBH" /><ref name="DBH amph primary" /> [[Flavin-containing monooxygenase 3|FMO3]]<ref name="Substituted amphetamines, FMO, and DBH" /><ref name="FMO" /><ref name="FMO3-Primary" /> |
|||
| metabolites = {{nowrap|[[4-hydroxyamphetamine]]}}, {{nowrap|[[4-hydroxynorephedrine]]}}, {{nowrap|[[4-hydroxyphenylacetone]]}}, [[benzoic acid]], [[hippuric acid]], [[norephedrine]], [[phenylacetone]]<ref name="FDA Pharmacokinetics" /><ref name="Metabolites"/> |
|||
| onset = {{abbr|IR|Immediate release}} dosing: {{nowrap|30–60}} minutes<ref name="Medscape Adderall Pharmacology">{{Cite encyclopedia|title = amphetamine/dextroamphetamine | section = Pharmacology |section-url = http://reference.medscape.com/drug/adderall-amphetamine-%20%20dextroamphetamine-342997#10 | website = Medscape | publisher = WebMD | access-date = 21 January 2016 | quote = Onset of action: 30–60 min }}</ref><br />{{abbr|XR|Extended release}} dosing: {{nowrap|1.5–2}} hours<ref name="Millichap: onset, peak, and duration">{{cite book | author = Millichap JG | editor = Millichap JG | title = Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD | year = 2010 | publisher = Springer | location = New York | isbn = 9781441913968 | pages = 112 | edition = 2nd | chapter = Chapter 9: Medications for ADHD | quote =<br />Table 9.2 Dextroamphetamine formulations of stimulant medication<br />Dexedrine [Peak:2–3 h] [Duration:5–6 h] ...<br />Adderall [Peak:2–3 h] [Duration:5–7 h]<br />Dexedrine spansules [Peak:7–8 h] [Duration:12 h] ...<br />Adderall XR [Peak:7–8 h] [Duration:12 h]<br />Vyvanse [Peak:3–4 h] [Duration:12 h]}}</ref><ref name="XR onset-duration">{{cite journal | vauthors = Brams M, Mao AR, Doyle RL | title = Onset of efficacy of long-acting psychostimulants in pediatric attention-deficit/hyperactivity disorder | journal =Postgraduate Medicine| volume = 120 | issue = 3 | pages = 69–88 | date = September 2008 | pmid = 18824827 | doi = 10.3810/pgm.2008.09.1909| s2cid = 31791162 }}</ref> |
|||
| elimination_half-life = {{nowrap|{{abbr|D-amph|dextroamphetamine}}}}: {{nowrap|9–11}} hours<ref name="FDA Pharmacokinetics" /><ref name="Adderall IR">{{cite web | title=Adderall- dextroamphetamine saccharate, amphetamine aspartate, dextroamphetamine sulfate, and amphetamine sulfate tablet | website=DailyMed | publisher = Teva Pharmaceuticals USA, Inc. | date=8 November 2019 | url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f22635fe-821d-4cde-aa12-419f8b53db81 | access-date=22 December 2019}}</ref><br />{{nowrap|{{abbr|L-amph|levoamphetamine}}}}: {{nowrap|11–14}} hours<ref name="FDA Pharmacokinetics" /><ref name="Adderall IR" /><br />[[pH]]-dependent: {{nowrap|7–34}} hours<ref name="HSDB Toxnet October 2017 Full archived record" /> |
|||
| duration_of_action = {{abbr|IR|Immediate release}} dosing: {{nowrap|3–6}} hours<ref name="Stahl's Essential Psychopharmacology" /><ref name="Millichap: onset, peak, and duration" /><ref name="Narcolepsy guide">{{cite journal | vauthors = Mignot EJ | title = A practical guide to the therapy of narcolepsy and hypersomnia syndromes | journal =Neurotherapeutics| volume = 9 | issue = 4 | pages = 739–752 | date = October 2012 | pmid = 23065655 | pmc = 3480574 | doi = 10.1007/s13311-012-0150-9 }}</ref><br /> {{abbr|XR|Extended release}} dosing: {{nowrap|8–12}} hours<ref name="Stahl's Essential Psychopharmacology" /><ref name="Millichap: onset, peak, and duration" /><ref name="Narcolepsy guide"/> |
|||
| excretion = Primarily [[renal]];<br />[[pH]]-dependent {{nowrap|range: 1–75%}}<ref name="FDA Pharmacokinetics" /> |
|||
<!--Identifiers-->| CAS_number = 300-62-9 |
|||
<!--Pharmacokinetic data--> |
|||
| CAS_number_Ref = {{cascite|correct|CAS}} |
|||
| bioavailability = nasal 75%; rectal 95–99%; intravenous 100% |
|||
| protein_bound = 15–40% |
|||
| metabolism = [[Hepatic]] ([[CYP2D6]])<ref>{{chú thích tạp chí |author=Miranda-G E, Sordo M, Salazar AM |title=Determination of amphetaminoe, methamphetamine, and hydroxyamphetamine derivatives in urine by gas chromatography-mass spectrometry and its relation to CYP2D6 phenotype of drug users |journal=J Anal Toxicol |volume=31 |issue=1 |pages=31–6 |year=2007 |pmid=17389081 |url=http://openurl.ingenta.com/content/nlm?genre=article&issn=0146-4760&volume=31&issue=1&spage=31&aulast=Miranda-G |access-date=2012-10-13 |archive-date=2020-05-03 |archive-url=https://web.archive.org/web/20200503052259/http://openurl.ingenta.com/content/nlm?genre=article&issn=0146-4760&volume=31&issue=1&spage=31&aulast=Miranda-G }}</ref> |
|||
| elimination_half-life = 12h average for d-isomer, 13h for l-isomer |
|||
| excretion = [[Renal]]; significant portion unaltered |
|||
<!--Identifiers--> |
|||
| CASNo_Ref = {{cascite|correct|CAS}} |
|||
| CAS_number_Ref = {{cascite|correct|??}} |
|||
| CAS_number = 300-62-9 |
|||
| CAS_supplemental = {{CAS|405-41-4}} |
|||
| ATC_prefix = N06 |
| ATC_prefix = N06 |
||
| ATC_suffix = BA01 |
| ATC_suffix = BA01 |
||
| ATC_supplemental = {{ATC|N06|BA02}} {{ATC|N06|BA12}} |
|||
| ChEBI_Ref = {{ebicite|changed|EBI}} |
|||
| ChEBI = 2679 |
|||
<!--Legal status-->| PubChem = 3007 |
|||
| StdInChI_Ref = {{stdinchicite|changed|chemspider}} |
|||
| IUPHAR_ligand = 4804 |
|||
| StdInChI = 1S/C9H13N/c1-8(10)7-9-5-3-2-4-6-9/h2-6,8H,7,10H2,1H3 |
|||
| StdInChIKey_Ref = {{stdinchicite|changed|chemspider}} |
|||
| StdInChIKey = KWTSXDURSIMDCE-UHFFFAOYSA-N |
|||
| PubChem = 3007 |
|||
| DrugBank_Ref = {{drugbankcite|correct|drugbank}} |
|||
| DrugBank = DB00182 |
| DrugBank = DB00182 |
||
| |
| DrugBank_Ref = {{drugbankcite|correct|drugbank}} |
||
| ChemSpiderID = 13852819 |
| ChemSpiderID = 13852819 |
||
| ChemSpiderID_Ref = {{chemspidercite|correct|chemspider}} |
|||
| NIAID_ChemDB = 018564 |
|||
| UNII_Ref = {{fdacite|correct|FDA}} |
|||
| UNII = CK833KGX7E |
| UNII = CK833KGX7E |
||
| |
| UNII_Ref = {{fdacite|correct|FDA}} |
||
| KEGG = D07445 |
| KEGG = D07445 |
||
| |
| KEGG_Ref = {{keggcite|correct|kegg}} |
||
| ChEBI = 2679 |
|||
| ChEBI_Ref = {{ebicite|correct|EBI}} |
|||
| ChEMBL = 405 |
| ChEMBL = 405 |
||
| ChEMBL_Ref = {{ebicite|correct|EBI}} |
|||
| NIAID_ChemDB = 018564 |
|||
| PDB_ligand =<!--Chemical and physical data--> |
|||
| synonyms = α-methylphenethylamine |
|||
| C = 9 |
|||
| H = 13 |
|||
| N = 1 |
|||
| SMILES = NC(C)Cc1ccccc1 |
|||
| StdInChI = 1S/C9H13N/c1-8(10)7-9-5-3-2-4-6-9/h2-6,8H,7,10H2,1H3 |
|||
| StdInChIKey = KWTSXDURSIMDCE-UHFFFAOYSA-N |
|||
| StdInChIKey_Ref = {{stdinchicite|correct|chemspider}} |
|||
| density =.936 |
|||
| density_notes = at 25 °C<ref name="PubChem - amphetamine density">{{cite encyclopedia | title=Amphetamine | section = Density | url = https://pubchem.ncbi.nlm.nih.gov/compound/amphetamine | section-url=https://pubchem.ncbi.nlm.nih.gov/compound/amphetamine#section=Density | work=PubChem Compound Database | publisher=United States National Library of Medicine – National Center for Biotechnology Information | access-date=9 November 2016 | date=5 November 2016}}</ref> |
|||
| StdInChI_Ref = {{stdinchicite|correct|chemspider}} |
|||
| melting_point = 11,3 |
|||
| melting_notes = (predicted)<ref name="Chemspider">{{cite encyclopedia | section-url=http://www.chemspider.com/Chemical-Structure.13852819.html | work=ChemSpider | publisher = Royal Society of Chemistry | title=Amphetamine | access-date=6 November 2013 | section=Properties: Predicted – EPISuite }}</ref> |
|||
| boiling_point = 203 |
|||
| boiling_notes = at 760 [[Millimeter of mercury|mmHg]]<ref name="Properties" /> |
|||
| verifiedrevid = 851154960 |
|||
}} |
|||
[[Category:Infobox drug articles with non-default infobox title|_]] |
|||
'''Amphetamin''' (hay còn gọi là '''hồng phiến''',<ref>{{Chú thích web|url=http://www.molisa.gov.vn:80/Pages/tintuc/chitiet.aspx?TinTucID=23352&page=368|tựa đề=Hãy coi Người nghiện ma túy là người bệnh|website=www.molisa.gov.vn|ngôn ngữ=en-US|ngày truy cập=2022-04-16}}</ref> viết tắt của <u>a</u>lpha-[[Methylphenethylamin|<u>m</u>ethyl<u>ph</u>en<u>et</u>hyl<u>amin</u>]], danh pháp theo tiếng Anh là '''Amphetamin''') là một [[chất kích thích]] hệ thần kinh trung [[Hệ thần kinh trung ương|ương]] (TKTW) mạnh được sử dụng trong điều trị [[rối loạn tăng động giảm chú ý]] (ADHD), [[chứng ngủ rũ]] và [[béo phì]]. Amphetamin được phát hiện vào năm 1887 và tồn tại dưới dạng hai [[chất đối quang]] (''enantiomer''): [[levoamphetamine|levoamphetamin]] và [[dextroamphetamine|dextroamphetamin]]. Danh pháp ''amphetamin'' đề cập đến hỗn hợp [[racemic]] chứa hai đồng phân đối quang ở dạng amin tinh khiết với tỷ lệ ngang nhau. Danh pháp này thường được sử dụng để chỉ hoặc là hỗn hợp hai chất đối quang, hoặc là chỉ một trong hai chất nêu trên. Cách dùng trên là quy ước không chính thức. Trong lịch sử, amphetamin được sử dụng để điều trị nghẹt mũi và trầm cảm. Amphetamin cũng được sử dụng là [[chất cải thiện khả năng thi đấu trong thể thao]], [[thuốc hưng trí]], [[thuốc kích dục]] và [[Hưng phấn|thuốc làm tăng hưng phấn]]. Amphetamin là [[thuốc theo toa]] ở nhiều quốc gia, và việc sở hữu và phân phối amphetamin được kiểm soát chặt chẽ do những nguy cơ to lớn của thuốc lên sức khỏe nếu việc [[Sử dụng thuốc giải trí|sử dụng thuốc phục vụ mục đích giải trí]]. {{#tag:ref|<ref name="Amph Uses" /><ref name="Proper definition">{{cite book | author = Yoshida T | editor = Klee H | title = Amphetamine Misuse: International Perspectives on Current Trends | date = 1997 | publisher = Harwood Academic Publishers | location = Amsterdam, Netherlands | isbn = 9789057020810 | page = [https://archive.org/details/amphetaminemisus0000unse/page/2 2] | chapter-url = https://books.google.com/books?id=gVw_wzZU4x8C&pg=PA2| chapter = Chapter 1: Use and Misuse of Amphetamines: An International Overview | quote = Amphetamine, in the singular form, properly applies to the racemate of 2-amino-1-phenylpropane. ... In its broadest context, however, the term [''amphetamines''] can even embrace a large number of structurally and pharmacologically related substances. | url = https://archive.org/details/amphetaminemisus0000unse/page/2 }}</ref><ref name="Malenka_2009" /><ref name="Ergogenics" /><ref name="FDA" /><ref name="Benzedrine" /><ref name="UN Convention" /><ref name="Nonmedical" /><ref name="Libido" /><ref name="MeSHAmphetamine">{{cite web | title = Amphetamine | url = https://www.nlm.nih.gov/cgi/mesh/2009/MB_cgi?mode=&term=Amphetamine | website = Medical Subject Headings | publisher = United States National Library of Medicine | access-date = 16 December 2013}}</ref><ref name="WHO INN active moiety">{{cite web | title = Guidelines on the Use of International Nonproprietary Names (INNS) for Pharmaceutical Substances | url = http://apps.who.int/medicinedocs/en/d/Jh1806e/2.4.html | archive-url = https://web.archive.org/web/20150109232455/http://apps.who.int/medicinedocs/en/d/Jh1806e/2.4.html | archive-date = 9 January 2015 | publisher = World Health Organization | access-date = 1 December 2014 | date = 1997 | quote = In principle, INNs are selected only for the active part of the molecule which is usually the base, acid or alcohol. In some cases, however, the active molecules need to be expanded for various reasons, such as formulation purposes, bioavailability or absorption rate. In 1975 the experts designated for the selection of INN decided to adopt a new policy for naming such molecules. In future, names for different salts or esters of the same active substance should differ only with regard to the inactive moiety of the molecule. ... The latter are called modified INNs (INNMs).}}</ref><ref name="Evekeo" />|group="sources"}} |
|||
Dược phẩm chứa hoạt chất amphetamin đầu tiên là Benzedrine, được chỉ định để điều trị nhiều loại bệnh. Hiện tại, các thành phẩm [[Amphetamin|amphetamin làm dược phẩm]] được kê đơn bao gồm: hỗn hợp racemic amphetamin, thuốc [[Adderall]], {{#tag:ref|The brand name '''Adderall''' is used throughout this article to refer to the amphetamine four-salt mixture it contains (dextroamphetamine sulfate 25%, dextroamphetamine saccharate 25%, amphetamine sulfate 25%, and amphetamine aspartate 25%). The nonproprietary name, which lists all four active constituent chemicals, is excessively lengthy.<ref name="NDCD">{{cite web | title = National Drug Code Amphetamine Search Results | url = https://www.accessdata.fda.gov/scripts/cder/ndc/results.cfm?beginrow=1&numberperpage=160&searchfield=amphetamine&searchtype=ActiveIngredient&OrderBy=ProprietaryName | website = National Drug Code Directory| publisher=United States Food and Drug Administration | access-date = 16 December 2013 | archive-url = https://web.archive.org/web/20131216080856/https://www.accessdata.fda.gov/scripts/cder/ndc/results.cfm?beginrow=1&numberperpage=160&searchfield=amphetamine&searchtype=ActiveIngredient&OrderBy=ProprietaryName | archive-date=16 December 2013 }}</ref>|name="UseOfAdderallName"|group="note"}} thuốc [[dextroamphetamin]], hoặc [[tiền chất]] không hoạt tính [[lisdexamfetamin]] [[Tiền chất|.]] Amphetamin làm tăng số lượng và [[Chất dẫn truyền thần kinh|kích thích]] tiết [[chất dẫn truyền thần kinh monoamin]] trong não, với tác dụng rõ rệt nhất là nhắm vào [[Chất dẫn truyền thần kinh|hệ thống dẫn truyền thần kinh]] [[Norepinephrine|noradrenalin]] và [[dopamin]].{{#tag:ref|<ref name="Amph Uses" /><ref name="Adderall IR" /><ref name="Malenka_2009" /><ref name="Benzedrine" /><ref name="Evekeo" /><ref name="Miller" /><ref name="Miller+Grandy 2016" />|group="sources"}} |
|||
Về mặt y học, ở liều điều trị, amphetamin gây ra các hiệu ứng về cảm xúc và nhận thức như [[hưng phấn]], thay đổi [[ham muốn tình dục]], tăng [[tỉnh táo]] và cải thiện khả năng [[kiểm soát nhận thức]]. Chất tác động về mặt thể chất như cải thiện thời gian đáp ứng, chống mệt mỏi và tăng sức mạnh cơ bắp. Liều amphetamin lớn hơn có thể làm suy giảm chức năng nhận thức và gây ra [[tiêu cơ vân]]. [[Nghiện]] là một tình trạng nghiêm trọng khi lạm dụng amphetamin để giải trí, nhưng ít có khả năng nghiện nếu sử dụng chất ở liều điều trị trong các cơ sở y tế. Liều rất cao có thể dẫn đến [[rối loạn tâm thần do chất kích thích]] (ví dụ, [[hoang tưởng]] (delusion) và [[Hoang tưởng ảo giác|tâm thần phân liệt thể paranoid]]), những rối loạn tâm thần này hiếm khi xảy ra ở liều điều trị ngay cả khi sử dụng lâu dài. Liều giải trí nói chung lớn hơn nhiều so với liều điều trị được chỉ định và có nguy cơ tác dụng phụ nghiêm trọng cao hơn nhiều.{{#tag:ref|<ref name="Adderall IR" /><ref name="Malenka_2009" /><ref name="Ergogenics" /><ref name="FDA" /><ref name="Libido" /><ref name="Westfall" /><ref name="Cochrane" /><ref name="Amphetamine-induced psychosis" /><ref name="Stimulant Misuse" /><ref name="Long-Term Outcomes Medications" /><ref name="NHMH_3e-Addiction doses" /><ref name="Addiction risk" />|group="sources"}} |
|||
Về mặt hóa học, amphetamin thuộc [[lớp phenethylamine]]. Đây là hợp chất gốc của lớp cấu trúc riêng mang tên [[amphetamine thay thế|amphetamin thay thế]], bao gồm các chất được biết đến nhiều như [[bupropion]], [[cathinon]], [[Thuốc lắc|MDMA]] (thuốc lắc) và [[methamphetamine|methamphetamin]] (ice, ma túy đá). Là một chất thuộc lớp phenethylamine, amphetamin cũng có liên quan về mặt hóa học với các [[chất điều biến thần kinh]] (''neuromodulator'') [[trace amine]] (là chất chủ vận [[TAAR1]]), cụ thể là [[Phenethylamin|phenethylamine]] và {{Nowrap|[[N-Methylphenethylamine|''N''-methylphenethylamine]]}}, cả hai đều được sản xuất trong cơ thể con người. Phenethylamine là hợp chất gốc của amphetamin, trong khi {{Nowrap|''N''-methylphenethylamine}} là [[đồng phân cấu tạo]] của amphetamin, chỉ khác nhau ở vị trí của [[nhóm methyl]]. |
|||
== Ứng dụng == |
|||
=== Y học === |
|||
Amphetamin được sử dụng để điều trị [[rối loạn tăng động giảm chú ý]] (ADHD), [[chứng ngủ rũ]] (rối loạn giấc ngủ) và [[béo phì]], và đôi khi được kê đơn {{Nowrap|[[off-label]]}} ([[kê đơn không theo hướng dẫn trên nhãn]]) cho các [[Chỉ định (y học)|chỉ định]] trước đây, đặc biệt là đối với [[trầm cảm kháng trị]] (trầm cảm không đáp ứng với thuốc) và [[Đau mãn tính|đau mạn tính]].<ref name="Stahl's Essential Psychopharmacology">{{Chú thích sách|title=Prescriber's Guide: Stahl's Essential Psychopharmacology|vauthors=Stahl SM|date=March 2017|publisher=Cambridge University Press|isbn=9781108228749|edition=6th|location=Cambridge, United Kingdom|pages=45–51|chapter=Amphetamine (D,L)|access-date=5 August 2017|chapter-url=https://books.google.com/books?id=9hssDwAAQBAJ&pg=PA45}}</ref><ref name="Evekeo">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f469fb38-0380-4621-9db3-a4f429126156|tựa đề=Evekeo- amphetamine sulfate tablet|ngày=14 August 2019|website=DailyMed|nhà xuất bản=Arbor Pharmaceuticals, LLC|ngày truy cập=22 December 2019}}</ref><ref name="Benzedrine sulfate">{{Chú thích tập san học thuật |vauthors=Bett WR |date=August 1946 |title=Benzedrine sulphate in clinical medicine; a survey of the literature |journal=Postgraduate Medical Journal |volume=22 |issue=250 |pages=205–218 |doi=10.1136/pgmj.22.250.205 |pmc=2478360 |pmid=20997404}}</ref> Phơi nhiễm với amphetamin lâu dài với liều lượng đủ cao ở một số loài động vật được cho là gây ra sự phát triển bất thường của [[Thụ thể dopamine|hệ dopamine]] hoặc tổn thương thần kinh,<ref name="pmid22392347">{{Chú thích tập san học thuật |vauthors=Carvalho M, Carmo H, Costa VM, Capela JP, Pontes H, Remião F, Carvalho F, Bastos Mde L |date=August 2012 |title=Toxicity of amphetamines: an update |journal=Archives of Toxicology |volume=86 |issue=8 |pages=1167–1231 |doi=10.1007/s00204-012-0815-5 |pmid=22392347}}</ref><ref name="AbuseAndAbnormalities">{{Chú thích tập san học thuật |vauthors=Berman S, O'Neill J, Fears S, Bartzokis G, London ED |date=October 2008 |title=Abuse of amphetamines and structural abnormalities in the brain |journal=Annals of the New York Academy of Sciences |volume=1141 |issue=1 |pages=195–220 |bibcode=<!-- No --> |doi=10.1196/annals.1441.031 |pmc=2769923 |pmid=18991959}}</ref> nhưng ở người bị ADHD, amphetamin dược phẩm ở liều lượng điều trị dường như cải thiện sự phát triển của não và tăng trưởng thần kinh.<ref name="Neuroplasticity 1">{{Chú thích tập san học thuật |vauthors=Hart H, Radua J, Nakao T, Mataix-Cols D, Rubia K |date=February 2013 |title=Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: exploring task-specific, stimulant medication, and age effects |journal=JAMA Psychiatry |volume=70 |issue=2 |pages=185–198 |doi=10.1001/jamapsychiatry.2013.277 |pmid=23247506 |doi-access=free}}</ref><ref name="Neuroplasticity 2">{{Chú thích tập san học thuật |vauthors=Spencer TJ, Brown A, Seidman LJ, Valera EM, Makris N, Lomedico A, Faraone SV, Biederman J |date=September 2013 |title=Effect of psychostimulants on brain structure and function in ADHD: a qualitative literature review of magnetic resonance imaging-based neuroimaging studies |journal=The Journal of Clinical Psychiatry |volume=74 |issue=9 |pages=902–917 |doi=10.4088/JCP.12r08287 |pmc=3801446 |pmid=24107764}}</ref><ref name="Neuroplasticity 3">{{Chú thích tập san học thuật |vauthors=Frodl T, Skokauskas N |date=February 2012 |title=Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects |journal=Acta Psychiatrica Scandinavica |volume=125 |issue=2 |pages=114–126 |doi=10.1111/j.1600-0447.2011.01786.x |pmid=22118249 |quote=Basal ganglia regions like the right globus pallidus, the right putamen, and the nucleus caudatus are structurally affected in children with ADHD. These changes and alterations in limbic regions like ACC and amygdala are more pronounced in non-treated populations and seem to diminish over time from child to adulthood. Treatment seems to have positive effects on brain structure. |doi-access=free}}</ref> Đánh giá các nghiên cứu [[chụp cộng hưởng từ]] (MRI) cho thấy rằng điều trị lâu dài với amphetamin làm giảm các bất thường trong cấu trúc và chức năng não ở những đối tượng mắc ADHD, và cải thiện chức năng ở một số phần của não, chẳng hạn như nhân đuôi phải của [[hạch nền]].<ref name="Neuroplasticity 1" /><ref name="Neuroplasticity 2" /><ref name="Neuroplasticity 3" /> |
|||
Các đánh giá về nghiên cứu chất kích thích trên lâm sàng đã xác định tính an toàn và hiệu quả của việc sử dụng amphetamin liên tục trong thời gian dài để điều trị ADHD.<ref name="Long-Term Outcomes Medications">{{Chú thích tập san học thuật |vauthors=Huang YS, Tsai MH |date=July 2011 |title=Long-term outcomes with medications for attention-deficit hyperactivity disorder: current status of knowledge |journal=CNS Drugs |volume=25 |issue=7 |pages=539–554 |doi=10.2165/11589380-000000000-00000 |pmid=21699268 |quote=Several other studies,<sup>[97-101]</sup> including a meta-analytic review<sup>[98]</sup> and a retrospective study,<sup>[97]</sup> suggested that stimulant therapy in childhood is associated with a reduced risk of subsequent substance use, cigarette smoking and alcohol use disorders. ... Recent studies have demonstrated that stimulants, along with the non-stimulants atomoxetine and extended-release guanfacine, are continuously effective for more than 2-year treatment periods with few and tolerable adverse effects. The effectiveness of long-term therapy includes not only the core symptoms of ADHD, but also improved quality of life and academic achievements. The most concerning short-term adverse effects of stimulants, such as elevated blood pressure and heart rate, waned in long-term follow-up studies. ... The current data do not support the potential impact of stimulants on the worsening or development of tics or substance abuse into adulthood. In the longest follow-up study (of more than 10 years), lifetime stimulant treatment for ADHD was effective and protective against the development of adverse psychiatric disorders.}}</ref><ref name="Millichap" /><ref name="Long-term 2015">{{Chú thích tập san học thuật |vauthors=Arnold LE, Hodgkins P, Caci H, Kahle J, Young S |date=February 2015 |title=Effect of treatment modality on long-term outcomes in attention-deficit/hyperactivity disorder: a systematic review |journal=PLOS ONE |volume=10 |issue=2 |pages=e0116407 |bibcode=<!-- No --> |doi=10.1371/journal.pone.0116407 |pmc=4340791 |pmid=25714373 |quote=The highest proportion of improved outcomes was reported with combination treatment (83% of outcomes). Among significantly improved outcomes, the largest effect sizes were found for combination treatment. The greatest improvements were associated with academic, self-esteem, or social function outcomes. |doi-access=free}}<br /><br />[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4340791/figure/pone.0116407.g003/ Figure 3: Treatment benefit by treatment type and outcome group]</ref> Các [[thử nghiệm ngẫu nhiên có đối chứng]] về liệu pháp kích thích liên tục để điều trị ADHD kéo dài 2 năm đã chứng minh hiệu quả điều trị và độ an toàn.<ref name="Long-Term Outcomes Medications" /><ref name="Millichap" /> Hai đánh giá đã chỉ ra rằng liệu pháp kích thích liên tục trong thời gian dài ở bệnh nhân ADHD có hiệu quả để giảm các triệu chứng chủ đạo của ADHD (gồm ''tăng động'', ''giảm chú ý'' và ''xung động''), nâng cao [[chất lượng cuộc sống]] và thành tích học tập, đồng thời cải thiện phần lớn các kết quả chức năng{{#tag:ref|The ADHD-related outcome domains with the greatest proportion of significantly improved outcomes from long-term continuous stimulant therapy include academics (≈55% of academic outcomes improved), driving (100% of driving outcomes improved), non-medical drug use (47% of addiction-related outcomes improved), obesity (≈65% of obesity-related outcomes improved), self-esteem (50% of self-esteem outcomes improved), and social function (67% of social function outcomes improved).<ref name="Long-term 2015" /><br /><br />The largest [[effect size]]s for outcome improvements from long-term stimulant therapy occur in the domains involving academics (e.g., [[grade point average]], achievement test scores, length of education, and education level), self-esteem (e.g., self-esteem questionnaire assessments, number of suicide attempts, and suicide rates), and social function (e.g., peer nomination scores, social skills, and quality of peer, family, and romantic relationships).<ref name="Long-term 2015" /><br /><br />Long-term combination therapy for ADHD (i.e., treatment with both a stimulant and behavioral therapy) produces even larger effect sizes for outcome improvements and improves a larger proportion of outcomes across each domain compared to long-term stimulant therapy alone.<ref name="Long-term 2015" />|group="note"}} dựa trên kết quả của 9 lĩnh vực, bao gồm: học vấn, hành vi chống đối xã hội, lái xe, sử dụng thuốc tùy tiện, béo phì, nghề nghiệp, lòng tự trọng, sử dụng dịch vụ (tức là các dịch vụ về học tập, nghề nghiệp, sức khỏe, tài chính và pháp lý) và chức năng xã hội.<ref name="Long-Term Outcomes Medications" /><ref name="Long-term 2015" /> Một thử nghiệm ngẫu nhiên có đối chứng kéo dài 9 tháng về điều trị bằng amphetamin cho ADHD ở trẻ em đã phát hiện ra mức tăng trung bình là 4,5 điểm [[Chỉ số thông minh|IQ]], cải thiện khả năng tập trung và tiếp tục giảm các hành vi gây rối và tăng động.<ref name="Millichap">{{Chú thích sách|title=Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD|last=Millichap JG|publisher=Springer|year=2010|isbn=9781441913968|editor-last=Millichap JG|edition=2nd|location=New York, USA|pages=121–123, 125–127|chapter=Chapter 9: Medications for ADHD|quote=Ongoing research has provided answers to many of the parents' concerns, and has confirmed the effectiveness and safety of the long-term use of medication.}}</ref> Một đánh giá khác chỉ ra rằng, dựa trên các [[nghiên cứu thuần tập]] có thời gian theo dõi dài nhất cho đến hiện tại, liệu pháp kích thích bắt đầu thực hiện từ lúc còn là trẻ nhỏ liên tục có hiệu quả để kiểm soát các triệu chứng ADHD và giảm nguy cơ tiến triển thành [[Rối loạn sử dụng chất gây nghiện|rối loạn tâm thần do sử dụng chất gây nghiện]] khi trưởng thành.<ref name="Long-Term Outcomes Medications" /> |
|||
Các mô hình hiện tại của ADHD cho thấy rằng bệnh có liên quan đến sự suy giảm chức năng trong một số [[Chất dẫn truyền thần kinh|hệ thống dẫn truyền thần kinh]] của não.<ref name="Malenka_2009_03" /> Những suy giảm chức năng này liên quan đến suy giảm chất dẫn truyền thần kinh [[Dopamin|dopamine]] trong [[con đường dopaminergic]] và chất dẫn truyền thần kinh [[Norepinephrine|noradrenalin]] trong con đường noradrenergic từ [[nhân lục]] (''locus coeruleus'') đến [[vỏ não trước trán]].<ref name="Malenka_2009_03" /> Các chất kích thích tâm lý như [[Methylphenidat|methylphenidate]] và amphetamin có hiệu quả trong điều trị ADHD vì chúng làm tăng hoạt động dẫn truyền thần kinh trong các hệ thống này.<ref name="Malenka_2009">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE|publisher=McGraw-Hill Medical|year=2009|isbn=9780071481274|veditors=Sydor A, Brown RY|edition=2nd|location=New York, USA|pages=318, 321|chapter=Chapter 13: Higher Cognitive Function and Behavioral Control|quote=Therapeutic (relatively low) doses of psychostimulants, such as methylphenidate and amphetamine, improve performance on working memory tasks both in normal subjects and those with ADHD. ... stimulants act not only on working memory function, but also on general levels of arousal and, within the nucleus accumbens, improve the saliency of tasks. Thus, stimulants improve performance on effortful but tedious tasks ... through indirect stimulation of dopamine and norepinephrine receptors. ...<br>Beyond these general permissive effects, dopamine (acting via D1 receptors) and norepinephrine (acting at several receptors) can, at optimal levels, enhance working memory and aspects of attention.}}</ref><ref name="Malenka_2009_03">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE|publisher=McGraw-Hill Medical|year=2009|isbn=9780071481274|veditors=Sydor A, Brown RY|edition=2nd|location=New York, USA|pages=154–157|chapter=Chapter 6: Widely Projecting Systems: Monoamines, Acetylcholine, and Orexin}}</ref><ref name="cognition enhancers">{{Chú thích tập san học thuật |vauthors=Bidwell LC, McClernon FJ, Kollins SH |date=August 2011 |title=Cognitive enhancers for the treatment of ADHD |journal=Pharmacology Biochemistry and Behavior |volume=99 |issue=2 |pages=262–274 |doi=10.1016/j.pbb.2011.05.002 |pmc=3353150 |pmid=21596055}}</ref> Khoảng 80% những người sử dụng các chất kích thích nêu trên cho thấy các triệu chứng ADHD được cải thiện.<ref name="Long-term 36">{{Chú thích tập san học thuật |vauthors=Parker J, Wales G, Chalhoub N, Harpin V |date=September 2013 |title=The long-term outcomes of interventions for the management of attention-deficit hyperactivity disorder in children and adolescents: a systematic review of randomized controlled trials |journal=Psychology Research and Behavior Management |volume=6 |pages=87–99 |doi=10.2147/PRBM.S49114 |pmc=3785407 |pmid=24082796 |quote=Only one paper<sup>53</sup> examining outcomes beyond 36 months met the review criteria. ... There is high level evidence suggesting that pharmacological treatment can have a major beneficial effect on the core symptoms of ADHD (hyperactivity, inattention, and impulsivity) in approximately 80% of cases compared with placebo controls, in the short term.}}</ref> Trẻ ADHD sử dụng thuốc kích thích nói chung có mối quan hệ tốt hơn với bạn bè đồng trang lứa và các thành viên trong gia đình, học giỏi hơn ở trường, ít mất tập trung và xung động hơn, đồng thời có thời gian chú ý lâu hơn.<ref name="Millichap_3">{{Chú thích sách|title=Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD|last=Millichap JG|publisher=Springer|year=2010|isbn=9781441913968|editor-last=Millichap JG|edition=2nd|location=New York, USA|pages=111–113|chapter=Chapter 9: Medications for ADHD}}</ref><ref name="ADHD">{{Chú thích web|url=http://www.webmd.com/add-adhd/childhood-adhd/stimulants-for-attention-deficit-hyperactivity-disorder|tựa đề=Stimulants for Attention Deficit Hyperactivity Disorder|ngày=12 April 2010|website=WebMD|nhà xuất bản=Healthwise|ngày truy cập=12 November 2013}}</ref> Trong tổng quan hệ thống của tổ chức Cochrane về việc điều trị ADHD ở trẻ em, thanh thiếu niên và người lớn bằng thuốc amphetamin cho thấy rằng các nghiên cứu thời gian ngắn đã chứng minh các loại thuốc này làm giảm mức độ nghiêm trọng của các triệu chứng, nhưng lại có tỷ lệ ngừng thuốc cao hơn so với các loại thuốc không gây kích thích do [[tác dụng phụ]] bất lợi của thuốc.<ref name="Cochrane Amphetamines ADHD">{{Chú thích tập san học thuật |vauthors=Castells X, Blanco-Silvente L, Cunill R |date=August 2018 |title=Amphetamines for attention deficit hyperactivity disorder (ADHD) in adults |journal=Cochrane Database of Systematic Reviews |volume=2018 |issue=8 |pages=CD007813 |doi=10.1002/14651858.CD007813.pub3 |pmc=6513464 |pmid=30091808}}</ref><ref name="pmid26844979">{{Chú thích tập san học thuật |vauthors=Punja S, Shamseer L, Hartling L, Urichuk L, Vandermeer B, Nikles J, Vohra S |date=February 2016 |title=Amphetamines for attention deficit hyperactivity disorder (ADHD) in children and adolescents |journal=Cochrane Database of Systematic Reviews |volume=2 |pages=CD009996 |doi=10.1002/14651858.CD009996.pub2 |pmid=26844979}}</ref> Tổng quan của Cochrane về điều trị ADHD ở trẻ em bị [[rối loạn tic]] như [[hội chứng Tourette]] chỉ ra rằng các chất kích thích nói chung không làm cho [[tic]] tồi tệ hơn, nhưng liều cao dextroamphetamin có thể làm trầm trọng thêm tic ở một số đối tượng.<ref name="pmid29944175">{{Chú thích tập san học thuật |vauthors=Osland ST, Steeves TD, Pringsheim T |date=June 2018 |title=Pharmacological treatment for attention deficit hyperactivity disorder (ADHD) in children with comorbid tic disorders |journal=Cochrane Database of Systematic Reviews |volume=2018 |issue=6 |pages=CD007990 |doi=10.1002/14651858.CD007990.pub3 |pmc=6513283 |pmid=29944175}}</ref> |
|||
=== Cải thiện các chức năng === |
|||
==== Cải thiện nhận thức ==== |
|||
Năm 2015, một [[tổng quan hệ thống]] và [[phân tích tổng hợp]] các [[thử nghiệm lâm sàng]] cho thấy rằng, khi được sử dụng ở liều thấp (liều điều trị), amphetamin cải thiện mặc dù ít nhưng vẫn đáng kể trong nhận thức, bao gồm [[trí nhớ hoạt động]] (''working memory''), [[trí nhớ từng hồi]] dài hạn (''long-term episodic memory''), [[kiểm soát ức chế]], và một số khía cạnh của [[Chú ý|sự chú ý]] ở người lớn khỏe mạnh bình thường;<ref name="Unambiguous PFC D1 A2">{{Chú thích tập san học thuật |vauthors=Spencer RC, Devilbiss DM, Berridge CW |date=June 2015 |title=The Cognition-Enhancing Effects of Psychostimulants Involve Direct Action in the Prefrontal Cortex |url=https://rdw.rowan.edu/cgi/viewcontent.cgi?article=1056&context=som_facpub |journal=Biological Psychiatry |volume=77 |issue=11 |pages=940–950 |doi=10.1016/j.biopsych.2014.09.013 |pmc=4377121 |pmid=25499957 |quote=The procognitive actions of psychostimulants are only associated with low doses. Surprisingly, despite nearly 80 years of clinical use, the neurobiology of the procognitive actions of psychostimulants has only recently been systematically investigated. Findings from this research unambiguously demonstrate that the cognition-enhancing effects of psychostimulants involve the preferential elevation of catecholamines in the PFC and the subsequent activation of norepinephrine α2 and dopamine D1 receptors. ... This differential modulation of PFC-dependent processes across dose appears to be associated with the differential involvement of noradrenergic α2 versus α1 receptors. Collectively, this evidence indicates that at low, clinically relevant doses, psychostimulants are devoid of the behavioral and neurochemical actions that define this class of drugs and instead act largely as cognitive enhancers (improving PFC-dependent function). ... In particular, in both animals and humans, lower doses maximally improve performance in tests of working memory and response inhibition, whereas maximal suppression of overt behavior and facilitation of attentional processes occurs at higher doses.}}</ref><ref name="Cognitive and motivational effects">{{Chú thích tập san học thuật |vauthors=Ilieva IP, Hook CJ, Farah MJ |date=June 2015 |title=Prescription Stimulants' Effects on Healthy Inhibitory Control, Working Memory, and Episodic Memory: A Meta-analysis |url=https://repository.upenn.edu/neuroethics_pubs/130 |journal=Journal of Cognitive Neuroscience |volume=27 |issue=6 |pages=1069–1089 |doi=10.1162/jocn_a_00776 |pmid=25591060 |quote=Specifically, in a set of experiments limited to high-quality designs, we found significant enhancement of several cognitive abilities. ... The results of this meta-analysis ... do confirm the reality of cognitive enhancing effects for normal healthy adults in general, while also indicating that these effects are modest in size.}}</ref> Những tác dụng tăng cường nhận thức này của amphetamin là do cơ chế trung gian: amphetamin là chất chủ vận, [[Chất chủ vận gián tiếp|kích hoạt gián tiếp]] đồng thời cả [[Thụ thể dopamine D1|thụ thể dopamine D<sub>1</sub>]] và [[Thụ thể alpha-2 adrenergic|thụ thể α<sub>2</sub> adrenergic]] ở [[vỏ não trước trán]].<ref name="Malenka_2009">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE|publisher=McGraw-Hill Medical|year=2009|isbn=9780071481274|veditors=Sydor A, Brown RY|edition=2nd|location=New York, USA|pages=318, 321|chapter=Chapter 13: Higher Cognitive Function and Behavioral Control|quote=Therapeutic (relatively low) doses of psychostimulants, such as methylphenidate and amphetamine, improve performance on working memory tasks both in normal subjects and those with ADHD. ... stimulants act not only on working memory function, but also on general levels of arousal and, within the nucleus accumbens, improve the saliency of tasks. Thus, stimulants improve performance on effortful but tedious tasks ... through indirect stimulation of dopamine and norepinephrine receptors. ...<br>Beyond these general permissive effects, dopamine (acting via D1 receptors) and norepinephrine (acting at several receptors) can, at optimal levels, enhance working memory and aspects of attention.}}</ref><ref name="Unambiguous PFC D1 A2" /> Một tổng quan hệ thống năm 2014 cho thấy liều lượng amphetamin thấp cũng cải thiện khả năng [[củng cố trí nhớ]], từ đó dẫn đến cải thiện khả năng [[Nhớ lại (thông tin)|nhớ lại thông tin]] (''recall'').<ref name="Cognition enhancement 2014 systematic review">{{Chú thích tập san học thuật |vauthors=Bagot KS, Kaminer Y |date=April 2014 |title=Efficacy of stimulants for cognitive enhancement in non-attention deficit hyperactivity disorder youth: a systematic review |journal=Addiction |volume=109 |issue=4 |pages=547–557 |doi=10.1111/add.12460 |pmc=4471173 |pmid=24749160 |quote=Amphetamine has been shown to improve consolidation of information (0.02 ≥ P ≤ 0.05), leading to improved recall.}}</ref> Liều điều trị của amphetamin cũng tăng cường hiệu quả dẫn truyền tại mạng lưới vỏ não, đây một tác dụng làm cải thiện trí nhớ hoạt động.<ref name="Malenka_2009" /><ref name="pmid11337538">{{Chú thích tập san học thuật |vauthors=Devous MD, Trivedi MH, Rush AJ |date=April 2001 |title=Regional cerebral blood flow response to oral amphetamine challenge in healthy volunteers |journal=Journal of Nuclear Medicine |volume=42 |issue=4 |pages=535–542 |pmid=11337538}}</ref> Amphetamin và các chất kích thích ADHD khác cũng cải thiện ''task saliency'' (''tạm dịch: sự nổi bật của nhiệm vụ'', thuật ngữ chỉ một quá trình nhận thức để giành sự tập trung chú ý để thúc đẩy, tạo động lực thực hiện và hoàn thành nhiệm vụ) và tăng [[tỉnh táo]], từ đó thúc đẩy hành vi hướng đến mục tiêu đã đề ra.<ref name="Malenka_2009" /><ref name="Malenka NAcc">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE|publisher=McGraw-Hill Medical|year=2009|isbn=9780071481274|veditors=Sydor A, Brown RY|edition=2nd|location=New York, USA|page=266|chapter=Chapter 10: Neural and Neuroendocrine Control of the Internal Milieu|quote=Dopamine acts in the nucleus accumbens to attach motivational significance to stimuli associated with reward.}}</ref><ref name="Continuum">{{Chú thích tập san học thuật |vauthors=Wood S, Sage JR, Shuman T, Anagnostaras SG |date=January 2014 |title=Psychostimulants and cognition: a continuum of behavioral and cognitive activation |journal=Pharmacological Reviews |volume=66 |issue=1 |pages=193–221 |doi=10.1124/pr.112.007054 |pmc=3880463 |pmid=24344115}}</ref> Các chất kích thích như amphetamin có thể cải thiện hiệu suất trong các nhiệm vụ khó khăn và nhàm chán. Có một số sinh viên sử dụng chất như một biện pháp hỗ trợ trong học tập và làm bài kiểm tra.<ref name="Malenka_2009">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE|publisher=McGraw-Hill Medical|year=2009|isbn=9780071481274|veditors=Sydor A, Brown RY|edition=2nd|location=New York, USA|pages=318, 321|chapter=Chapter 13: Higher Cognitive Function and Behavioral Control|quote=Therapeutic (relatively low) doses of psychostimulants, such as methylphenidate and amphetamine, improve performance on working memory tasks both in normal subjects and those with ADHD. ... stimulants act not only on working memory function, but also on general levels of arousal and, within the nucleus accumbens, improve the saliency of tasks. Thus, stimulants improve performance on effortful but tedious tasks ... through indirect stimulation of dopamine and norepinephrine receptors. ...<br>Beyond these general permissive effects, dopamine (acting via D1 receptors) and norepinephrine (acting at several receptors) can, at optimal levels, enhance working memory and aspects of attention.}}<cite class="citation book cs1" data-ve-ignore="true" id="CITEREFMalenkaNestlerHyman2009">Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 13: Higher Cognitive Function and Behavioral Control". In Sydor A, Brown RY (eds.). ''Molecular Neuropharmacology: A Foundation for Clinical Neuroscience'' (2nd ed.). New York, USA: McGraw-Hill Medical. pp. 318, 321. [[ISBN]] [[Special:BookSources/9780071481274|<bdi>9780071481274</bdi>]].<q>Therapeutic (relatively low) doses of psychostimulants, such as methylphenidate and amphetamine, improve performance on working memory tasks both in normal subjects and those with ADHD. ... stimulants act not only on working memory function, but also on general levels of arousal and, within the nucleus accumbens, improve the saliency of tasks. Thus, stimulants improve performance on effortful but tedious tasks ... through indirect stimulation of dopamine and norepinephrine receptors. ...<br /><br />Beyond these general permissive effects, dopamine (acting via D1 receptors) and norepinephrine (acting at several receptors) can, at optimal levels, enhance working memory and aspects of attention.</q></cite></ref><ref name="Continuum" /><ref name="Test taking aid">{{Chú thích web|url=http://www.jsonline.com/story/index.aspx?id=410902|tựa đề=Pills become an addictive study aid|tác giả=Twohey M|ngày=26 March 2006|website=JS Online|url lưu trữ=https://web.archive.org/web/20070815200239/http://www.jsonline.com/story/index.aspx?id=410902|ngày lưu trữ=15 August 2007|ngày truy cập=2 December 2007}}</ref> Dựa trên các nghiên cứu về việc sử dụng chất kích thích bất hợp pháp tự báo cáo, {{Nowrap|5–35%}} sinh viên đại học sử dụng chất kích thích chủ yếu được sử dụng để nâng cao thành tích học tập chứ không phải là để chơi bời, tiêu khiển.<ref name="pmid16999660">{{Chú thích tập san học thuật |vauthors=Teter CJ, McCabe SE, LaGrange K, Cranford JA, Boyd CJ |date=October 2006 |title=Illicit use of specific prescription stimulants among college students: prevalence, motives, and routes of administration |journal=Pharmacotherapy |volume=26 |issue=10 |pages=1501–1510 |doi=10.1592/phco.26.10.1501 |pmc=1794223 |pmid=16999660}}</ref><ref name="Diversion prevalence 1">{{Chú thích tập san học thuật |vauthors=Weyandt LL, Oster DR, Marraccini ME, Gudmundsdottir BG, Munro BA, Zavras BM, Kuhar B |date=September 2014 |title=Pharmacological interventions for adolescents and adults with ADHD: stimulant and nonstimulant medications and misuse of prescription stimulants |journal=Psychology Research and Behavior Management |volume=7 |pages=223–249 |doi=10.2147/PRBM.S47013 |pmc=4164338 |pmid=25228824 |quote=misuse of prescription stimulants has become a serious problem on college campuses across the US and has been recently documented in other countries as well. ... Indeed, large numbers of students claim to have engaged in the nonmedical use of prescription stimulants, which is reflected in lifetime prevalence rates of prescription stimulant misuse ranging from 5% to nearly 34% of students.}}</ref><ref name="Diversion prevalence 2">{{Chú thích tập san học thuật |vauthors=Clemow DB, Walker DJ |date=September 2014 |title=The potential for misuse and abuse of medications in ADHD: a review |journal=Postgraduate Medicine |volume=126 |issue=5 |pages=64–81 |doi=10.3810/pgm.2014.09.2801 |pmid=25295651 |quote=Overall, the data suggest that ADHD medication misuse and diversion are common health care problems for stimulant medications, with the prevalence believed to be approximately 5% to 10% of high school students and 5% to 35% of college students, depending on the study.}}</ref> Tuy nhiên, liều amphetamin cao trên liều điều trị có thể ảnh hưởng đến trí nhớ hoạt động và các khía cạnh khác của kiểm soát nhận thức.<ref name="Malenka_2009" /><ref name="Continuum" /> |
|||
==== Cải thiện thể chất ==== |
|||
Amphetamin được một số vận động viên sử dụng vì tác dụng cải thiện thể chất, chẳng hạn như tăng sức bền và sự tỉnh táo;<ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref> Tuy nhiên, các cơ quan chống doping của quốc gia và quốc tế đã cấm việc sử dụng amphetamin ngoài mục đích y tế tại các sự kiện thể thao.<ref name="NCAA">{{Chú thích web|url=http://www.ncaapublications.com/productdownloads/SAHS09.pdf|tựa đề=National Study of Substance Use Trends Among NCAA College Student-Athletes|tác giả=Bracken NM|ngày=January 2012|website=NCAA Publications|nhà xuất bản=National Collegiate Athletic Association|url lưu trữ=https://ghostarchive.org/archive/20221009/http://www.ncaapublications.com/productdownloads/SAHS09.pdf|ngày lưu trữ=2022-10-09|url-status=live|ngày truy cập=8 October 2013}}</ref><ref name="WADA & AD regulation">{{Chú thích tập san học thuật |last=Docherty JR |date=June 2008 |title=Pharmacology of stimulants prohibited by the World Anti-Doping Agency (WADA) |journal=British Journal of Pharmacology |volume=154 |issue=3 |pages=606–622 |doi=10.1038/bjp.2008.124 |pmc=2439527 |pmid=18500382}}</ref> Ở những người khỏe mạnh với liều điều trị bằng đường uống, amphetamin đã được chứng minh là làm tăng [[sức mạnh thể chất]], tăng tốc độ di chuyển, cải thiện thể chất, hoạt động trong các bài tập kỵ khí (còn gọi là bài tập yếm khí) và bài tập [[sức bền]] (tức là thuốc làm trì hoãn sự [[mệt mỏi]] khi tập các bài tập này), đồng thời cải thiện thời gian đáp ứng (bằng cách [[đo thời gian tâm lý]], ''mental chronometry'').<ref name="Ergogenics2" /><ref name="Roelands_2013" /> Amphetamin cải thiện sức bền và thời gian đáp ứng chủ yếu thông qua [[ức chế tái hấp thu]] và giải phóng dopamine trong hệ TKTW.<ref name="Ergogenics2" /><ref name="Roelands_2013">{{Chú thích tập san học thuật |vauthors=Roelands B, de Koning J, Foster C, Hettinga F, Meeusen R |date=May 2013 |title=Neurophysiological determinants of theoretical concepts and mechanisms involved in pacing |journal=Sports Medicine |volume=43 |issue=5 |pages=301–311 |doi=10.1007/s40279-013-0030-4 |pmid=23456493 |quote=In high-ambient temperatures, dopaminergic manipulations clearly improve performance. The distribution of the power output reveals that after dopamine reuptake inhibition, subjects are able to maintain a higher power output compared with placebo. ... Dopaminergic drugs appear to override a safety switch and allow athletes to use a reserve capacity that is 'off-limits' in a normal (placebo) situation.}}</ref><ref name="Amph-DA reaction time">{{Chú thích tập san học thuật |vauthors=Parker KL, Lamichhane D, Caetano MS, Narayanan NS |date=October 2013 |title=Executive dysfunction in Parkinson's disease and timing deficits |journal=Frontiers in Integrative Neuroscience |volume=7 |page=75 |doi=10.3389/fnint.2013.00075 |pmc=3813949 |pmid=24198770 |quote=Manipulations of dopaminergic signaling profoundly influence interval timing, leading to the hypothesis that dopamine influences internal pacemaker, or "clock," activity. For instance, amphetamine, which increases concentrations of dopamine at the synaptic cleft advances the start of responding during interval timing, whereas antagonists of D2 type dopamine receptors typically slow timing;... Depletion of dopamine in healthy volunteers impairs timing, while amphetamine releases synaptic dopamine and speeds up timing. |doi-access=free}}</ref> Amphetamin và các loại thuốc dopaminergic khác cũng làm tăng nguồn năng lượng phục vụ cho hoạt động gắng sức bằng cách cho phép [[Nhiệt độ cơ thể con người|tăng ngưỡng thân nhiệt]] để đạt được khả năng hoạt động mà nếu không sử dụng thuốc thì đây là những hoạt động quá giới hạn, không thể làm được.<ref name="Roelands_2013" /><ref name="Central mechanisms affecting exertion">{{Chú thích tập san học thuật |vauthors=Rattray B, Argus C, Martin K, Northey J, Driller M |date=March 2015 |title=Is it time to turn our attention toward central mechanisms for post-exertional recovery strategies and performance? |journal=Frontiers in Physiology |volume=6 |pages=79 |doi=10.3389/fphys.2015.00079 |pmc=4362407 |pmid=25852568 |quote=Aside from accounting for the reduced performance of mentally fatigued participants, this model rationalizes the reduced RPE and hence improved cycling time trial performance of athletes using a glucose mouthwash (Chambers et al., 2009) and the greater power output during a RPE matched cycling time trial following amphetamine ingestion (Swart, 2009). ... Dopamine stimulating drugs are known to enhance aspects of exercise performance (Roelands et al., 2008) |doi-access=free}}</ref><ref name="Monoamine+drug effects on exercise - fatigue and heat">{{Chú thích tập san học thuật |vauthors=Roelands B, De Pauw K, Meeusen R |date=June 2015 |title=Neurophysiological effects of exercise in the heat |journal=Scandinavian Journal of Medicine & Science in Sports |volume=25 |issue=Suppl 1 |pages=65–78 |doi=10.1111/sms.12350 |pmid=25943657 |quote=This indicates that subjects did not feel they were producing more power and consequently more heat. The authors concluded that the "safety switch" or the mechanisms existing in the body to prevent harmful effects are overridden by the drug administration (Roelands et al., 2008b). Taken together, these data indicate strong ergogenic effects of an increased DA concentration in the brain, without any change in the perception of effort.}}</ref> Ở liều điều trị, tác dụng phụ của amphetamin không ảnh hưởng đến hoạt động thể thao;<ref name="Ergogenics2" /> Tuy nhiên, ở liều lượng cao hơn nhiều lần liều điều trị, amphetamin có thể gây ra các tác động làm suy giảm thể chất nghiêm trọng do làm [[tiêu cơ vân]] (tức là phân hủy cơ) và [[tăng thân nhiệt]].<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref name="Ergogenics2">{{Chú thích tập san học thuật |last=Parr JW |date=July 2011 |title=Attention-deficit hyperactivity disorder and the athlete: new advances and understanding |journal=Clinics in Sports Medicine |volume=30 |issue=3 |pages=591–610 |doi=10.1016/j.csm.2011.03.007 |pmid=21658550 |quote=In 1980, Chandler and Blair<sup>47</sup> showed significant increases in knee extension strength, acceleration, anaerobic capacity, time to exhaustion during exercise, pre-exercise and maximum heart rates, and time to exhaustion during maximal oxygen consumption (VO2 max) testing after administration of 15 mg of dextroamphetamine versus placebo. Most of the information to answer this question has been obtained in the past decade through studies of fatigue rather than an attempt to systematically investigate the effect of ADHD drugs on exercise.}}</ref> |
|||
== Chống chỉ định == |
|||
Theo Chương trình Quốc tế về An toàn Hóa chất (IPCS) và [[Cục quản lý Thực phẩm và Dược phẩm Hoa Kỳ|Cục Quản lý Thực phẩm và Dược phẩm Hoa Kỳ]] (USFDA), [note 8] [[chống chỉ định]] amphetamin ở những người có tiền sử [[lạm dụng chất]], [[bệnh tim mạch]], kích động nặng, hoặc quá lo lắng.<ref name="Evekeo">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f469fb38-0380-4621-9db3-a4f429126156|tựa đề=Evekeo- amphetamine sulfate tablet|ngày=14 August 2019|website=DailyMed|nhà xuất bản=Arbor Pharmaceuticals, LLC|ngày truy cập=22 December 2019}}</ref><ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref> Chất cũng được chống chỉ định ở những người bị [[xơ cứng động mạch]], [[Cườm nước|glôcôm]] (tăng nhãn áp), [[cường giáp]] (tiết quá nhiều hormone tuyến giáp), hoặc [[Cao huyết áp|tăng huyết áp]] từ trung bình đến nặng.<ref name="Evekeo" /><ref name="FDA" /> Các tổ chức này chỉ ra rằng những người đã trải qua [[Quá mẫn|phản ứng quá mẫn]] với các chất kích thích khác, hoặc đang dùng [[chất ức chế monoamin oxidase]] (MAOI) không nên dùng amphetamin,<ref name="Evekeo" /><ref name="FDA" /> mặc dù việc sử dụng đồng thời amphetamin và chất ức chế monoamine oxidase đã được ghi nhận là an toàn.<ref name="Review MAOI-amph">{{Chú thích tập san học thuật |vauthors=Feinberg SS |date=November 2004 |title=Combining stimulants with monoamine oxidase inhibitors: a review of uses and one possible additional indication |journal=The Journal of Clinical Psychiatry |volume=65 |issue=11 |pages=1520–1524 |doi=10.4088/jcp.v65n1113 |pmid=15554766}}</ref><ref name="Primary MAOI-amph">{{Chú thích tập san học thuật |vauthors=Stewart JW, Deliyannides DA, McGrath PJ |date=June 2014 |title=How treatable is refractory depression? |journal=Journal of Affective Disorders |volume=167 |pages=148–152 |doi=10.1016/j.jad.2014.05.047 |pmid=24972362}}</ref> Các tổ chức này cũng khuyến cáo rằng bất kỳ ai mắc [[chán ăn tâm thần]], [[rối loạn lưỡng cực]], trầm cảm, tăng huyết áp, chức năng gan hoặc thận bất thường, [[hưng cảm]], [[Loạn tâm thần|loạn thần]], [[hội chứng Raynaud]], [[cơn động kinh]], các vấn đề về [[tuyến giáp]], [[tic]] hay [[hội chứng Tourette]] nên theo dõi các triệu chứng trong khi dùng amphetamin.<ref name="FDA" /> Bằng chứng từ các nghiên cứu trên người chỉ ra rằng việc sử dụng amphetamin điều trị không gây ra các bất thường về phát triển ở thai nhi hoặc trẻ sơ sinh (tức là amphetamin không [[Quái thai học|gây quái thai]] ở người), nhưng lạm dụng amphetamin có thể gây ra rủi ro cho thai nhi. Amphetamin cũng đã được chứng minh là có khả năng đi vào sữa mẹ, vì vậy hai tổ chức IPCS và USFDA khuyên các bà mẹ tránh cho con bú khi sử dụng thuốc.<ref name="FDA" /> Do khả năng gây suy giảm tăng trưởng thể chất có hồi phục, USFDA khuyến nghị nên theo dõi chiều cao và cân nặng của trẻ em và thanh thiếu niên khi trẻ được kê toa một loại dược phẩm chứa amphetamin.<ref name="FDA" /> |
|||
== Tác dụng phụ == |
|||
Amphetamin có rất nhiều [[Tác dụng bất lợi|tác dụng phụ bất lợi]] và có tính đa dạng. Liều lượng amphetamin được sử dụng là yếu tố chính để xác định khả năng xảy ra và mức độ nghiêm trọng của các tác dụng phụ.<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref> Các chế phẩm amphetamin như [[Adderall]], Dexedrine, và các sản phẩm tương đương hiện được USFDA chấp thuận để sử dụng điều trị lâu dài.<ref name="FDA" /> [[Sử dụng thuốc giải trí|Sử dụng amphetamin để giải trí]] thường có liều lượng lớn hơn nhiều so với liều điều trị, có nguy cơ gây tác dụng phụ nghiêm trọng hơn so với liều lượng được sử dụng cho mục đích điều trị.<ref name="Westfall" /> |
|||
=== Về mặt thể chất === |
|||
Tác dụng phụ trên [[Hệ tuần hoàn|tim mạch]] bao gồm [[tăng huyết áp]] hay [[Huyết áp thấp|tụt huyết áp]] do [[ngất phế vị]] (ngất do phản xạ thần kinh phế vị hay [[thần kinh lang thang]]), [[hội chứng Raynaud]] (giảm lưu lượng máu đến bàn tay và bàn chân), và [[Nhịp tim nhanh bất thường|nhịp tim nhanh]].<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref><ref name="pmid18295156">{{Chú thích tập san học thuật |last=Vitiello B |date=April 2008 |title=Understanding the risk of using medications for attention deficit hyperactivity disorder with respect to physical growth and cardiovascular function |journal=Child and Adolescent Psychiatric Clinics of North America |volume=17 |issue=2 |pages=459–474 |doi=10.1016/j.chc.2007.11.010 |pmc=2408826 |pmid=18295156}}</ref> Tác dụng phụ về tình dục ở nam giới gồm [[rối loạn cường dương]]: cương cứng thường xuyên hoặc [[Chứng cương đau|cương cứng kéo dài]].<ref name="FDA" /> Tác dụng phụ về đường tiêu hóa gồm [[đau bụng]], [[táo bón]], [[tiêu chảy]] và [[buồn nôn]].<ref name="Stahl's Essential Psychopharmacology">{{Chú thích sách|title=Prescriber's Guide: Stahl's Essential Psychopharmacology|vauthors=Stahl SM|date=March 2017|publisher=Cambridge University Press|isbn=9781108228749|edition=6th|location=Cambridge, United Kingdom|pages=45–51|chapter=Amphetamine (D,L)|access-date=5 August 2017|chapter-url=https://books.google.com/books?id=9hssDwAAQBAJ&pg=PA45}}</ref><ref name="FDA" /> Tác dụng phụ về thể chất khác bao gồm [[chán ăn]], [[mờ mắt]], [[khô miệng]], [[Nghiến răng|nghiến răng quá mức]], chảy máu cam, đổ mồ hôi nhiều, [[viêm mũi do thuốc]], giảm [[ngưỡng co giật]], rối loạn [[tic]] (một dạng rối loạn vận động) và [[giảm cân]]. Các tác dụng phụ nguy hiểm về thể chất hiếm khi xảy ra khi dùng ở liều điều trị.<ref name="Westfall" /> |
|||
Amphetamin kích thích [[trung tâm hô hấp]] ở [[hành não]], làm thở nhanh và sâu hơn.<ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref> Ở người bình thường ở liều điều trị, tác dụng này thường ít để ý, nhưng ở bệnh nhân có tổn thương hô hấp, tác dụng trên có thể biểu hiện rõ.<ref name="Westfall" /> Amphetamin cũng gây ra [[Co cơ|co thắt]] [[Cơ vòng bàng quang|cơ vòng ở bàng quang]], (cơ kiểm soát việc đi tiểu), có thể gây [[bí tiểu]].<ref name="Westfall" /> Tác dụng phụ này có thể hữu ích trong việc điều trị [[đái dầm]] và [[tiểu tiện không tự chủ]].<ref name="Westfall" /> không đoán trước được tác dụng của amphetamin trên đường tiêu hóa.<ref name="Westfall" /> Amphetamin có thể làm giảm nhu động ruột (liên quan tới tốc độ di chuyển của thức ăn qua hệ tiêu hóa);<ref name="Westfall" /> tuy nhiên, amphetamin có thể làm tăng nhu động khi làm giãn [[cơ trơn]] đường tiêu hóa.<ref name="Westfall" /> Amphetamin cũng có [[Thuốc giảm đau|tác dụng giảm đau]] nhẹ và có thể hiệp dồng với tác dụng giảm đau của [[Thuốc giảm đau nhóm opioid|nhóm opioid]].<ref name="Stahl's Essential Psychopharmacology">{{Chú thích sách|title=Prescriber's Guide: Stahl's Essential Psychopharmacology|vauthors=Stahl SM|date=March 2017|publisher=Cambridge University Press|isbn=9781108228749|edition=6th|location=Cambridge, United Kingdom|pages=45–51|chapter=Amphetamine (D,L)|access-date=5 August 2017|chapter-url=https://books.google.com/books?id=9hssDwAAQBAJ&pg=PA45}}</ref><ref name="Westfall" /> |
|||
Các nghiên cứu do USFDA ủy quyền từ năm 2011 ở trẻ em, trẻ vị thành niên và người lớn chỉ ra rằng không có mối liên quan giữa các biến cố tim mạch nghiêm trọng ([[Ngừng tim|đột tử]], [[Nhồi máu cơ tim|đau tim]] và [[Tai biến mạch máu não|đột quỵ]]) với việc sử dụng amphetamin hoặc các chất kích thích ADHD khác trong y tế. [sources 6] Tuy nhiên, dược phẩm amphetamin có [[chống chỉ định]] ở những người mắc [[bệnh tim mạch]]. |
|||
=== Về mặt tâm lý === |
|||
Ở liều điều trị bình thường, các tác dụng phụ về mặt tâm lý phổ biến nhất của amphetamin gồm tăng [[cảnh giác]], lo lắng, tăng độ tập trung, tính chủ động, [[tự tin]] và hòa đồng, thay đổi khí sắc ([[Hưng phấn|khí sắc tăng]] sau đó là [[khí sắc trầm]] mức độ nhẹ), [[mất ngủ]], [[tỉnh táo]] và giảm cảm giác mệt mỏi.<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref> Các tác dụng phụ ít phổ biến hơn bao gồm [[Lo âu|lo lắng]], thay đổi [[ham muốn tình dục]], tính cách mạnh mẽ, cáu kỉnh, hành vi lặp đi lặp lại hoặc ám ảnh và bồn chồn; những tác động này phụ thuộc vào tính cách cá nhân và trạng thái tinh thần hiện tại của bệnh nhân.<ref name="Westfall" /> Có nguy cơ [[Rối loạn tâm thần do chất kích thích|rối loạn tâm thần do amphetamin]] (ví dụ, [[hoang tưởng]] và [[Hoang tưởng ảo giác|tâm thần phân liệt thể paranoid]]).<ref name="FDA" /><ref name="Amphetamine-induced psychosis">{{Chú thích tập san học thuật |vauthors=Bramness JG, Gundersen ØH, Guterstam J, Rognli EB, Konstenius M, Løberg EM, Medhus S, Tanum L, Franck J |date=December 2012 |title=Amphetamine-induced psychosis—a separate diagnostic entity or primary psychosis triggered in the vulnerable? |journal=BMC Psychiatry |volume=12 |pages=221 |doi=10.1186/1471-244X-12-221 |pmc=3554477 |pmid=23216941 |quote=In these studies, amphetamine was given in consecutively higher doses until psychosis was precipitated, often after 100–300 mg of amphetamine ... Secondly, psychosis has been viewed as an adverse event, although rare, in children with ADHD who have been treated with amphetamine}}</ref> Rối loạn tâm thần này cũng có thể xảy ra ở liều điều trị nếu thời gian điều trị lâu dài.<ref name="FDA" /><ref name="Amphetamine-induced psychosis" /><ref name="Stimulant Misuse">{{Chú thích web|url=http://www.acha.org/prof_dev/ADHD_docs/ADHD_PDprogram_Article2.pdf|tựa đề=Stimulant Misuse: Strategies to Manage a Growing Problem|tác giả=Greydanus D|website=American College Health Association|nhà xuất bản=ACHA Professional Development Program|trang=20|kiểu=Review Article|url lưu trữ=https://web.archive.org/web/20131103155156/http://www.acha.org/prof_dev/ADHD_docs/ADHD_PDprogram_Article2.pdf|ngày lưu trữ=3 November 2013|ngày truy cập=2 November 2013}}</ref> Theo USFDA, "không có bằng chứng hệ thống" cho thấy chất kích thích tạo ra hành vi hung hăng hoặc thù địch.<ref name="FDA" /> |
|||
Amphetamin cũng được chứng minh là tạo ra [[ưa thích nơi chốn có điều kiện]] (''conditioned place preference'')<ref>Thuật ngữ lấy từ:<nowiki>[https://mlearning.hoasen.edu.vn/pluginfile.php/60438/mod_resource/content/1/Ba%CC%80i%203%20-%20%C4%90ie%CC%82%CC%80u%20kie%CC%A3%CC%82n%20hoa%CC%81%20pha%CC%89n%20ho%CC%82%CC%80i.pdf]</nowiki></ref> ở bệnh nhân tuân theo liều điều trị,<ref name="Cochrane Amphetamines ADHD">{{Chú thích tập san học thuật |vauthors=Castells X, Blanco-Silvente L, Cunill R |date=August 2018 |title=Amphetamines for attention deficit hyperactivity disorder (ADHD) in adults |journal=Cochrane Database of Systematic Reviews |volume=2018 |issue=8 |pages=CD007813 |doi=10.1002/14651858.CD007813.pub3 |pmc=6513464 |pmid=30091808}}</ref><ref name="Human CPP">{{Chú thích tập san học thuật |vauthors=Childs E, de Wit H |date=May 2009 |title=Amphetamine-induced place preference in humans |journal=Biological Psychiatry |volume=65 |issue=10 |pages=900–904 |doi=10.1016/j.biopsych.2008.11.016 |pmc=2693956 |pmid=19111278 |quote=This study demonstrates that humans, like nonhumans, prefer a place associated with amphetamine administration. These findings support the idea that subjective responses to a drug contribute to its ability to establish place conditioning.}}</ref> có nghĩa là bệnh nhân thích dành thời gian đi đến những nơi trước đây họ sử dụng amphetamin tại đó.<ref name="Human CPP" /> |
|||
=== Rối loạn tăng cường === |
|||
==== Nghiện ==== |
|||
{{Thuật ngữ nghiện|collapse=y|width=610px}} {{Transcription factor glossary|collapse=y|width=610px}}{{Psychostimulant addiction|align=right|header=[[Signaling cascade]] in the [[nucleus accumbens]] that results in amphetamine addiction}}{{Psychostimulant addiction|align=right|header=[[Signaling cascade]] in the [[nucleus accumbens]] that results in amphetamine addiction}}[[Nghiện]] là tác hại nghiêm trọng khi sử dụng amphetamin để giải trí, nhưng ít có khả năng xảy ra khi sử dụng lâu dài ở liều điều trị;<ref name="Long-Term Outcomes Medications">{{Chú thích tập san học thuật |vauthors=Huang YS, Tsai MH |date=July 2011 |title=Long-term outcomes with medications for attention-deficit hyperactivity disorder: current status of knowledge |journal=CNS Drugs |volume=25 |issue=7 |pages=539–554 |doi=10.2165/11589380-000000000-00000 |pmid=21699268 |quote=Several other studies,<sup>[97-101]</sup> including a meta-analytic review<sup>[98]</sup> and a retrospective study,<sup>[97]</sup> suggested that stimulant therapy in childhood is associated with a reduced risk of subsequent substance use, cigarette smoking and alcohol use disorders. ... Recent studies have demonstrated that stimulants, along with the non-stimulants atomoxetine and extended-release guanfacine, are continuously effective for more than 2-year treatment periods with few and tolerable adverse effects. The effectiveness of long-term therapy includes not only the core symptoms of ADHD, but also improved quality of life and academic achievements. The most concerning short-term adverse effects of stimulants, such as elevated blood pressure and heart rate, waned in long-term follow-up studies. ... The current data do not support the potential impact of stimulants on the worsening or development of tics or substance abuse into adulthood. In the longest follow-up study (of more than 10 years), lifetime stimulant treatment for ADHD was effective and protective against the development of adverse psychiatric disorders.}}</ref><ref name="NHMH_3e-Addiction doses">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE, Holtzman DM|publisher=McGraw-Hill Medical|year=2015|isbn=9780071827706|edition=3rd|location=New York|chapter=Chapter 16: Reinforcement and Addictive Disorders|quote=Such agents also have important therapeutic uses; cocaine, for example, is used as a local anesthetic (Chapter 2), and amphetamines and methylphenidate are used in low doses to treat attention deficit hyperactivity disorder and in higher doses to treat narcolepsy (Chapter 12). Despite their clinical uses, these drugs are strongly reinforcing, and their long-term use at high doses is linked with potential addiction, especially when they are rapidly administered or when high-potency forms are given.}}</ref><ref name="Addiction risk">{{Chú thích tập san học thuật |vauthors=Kollins SH |date=May 2008 |title=A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders |journal=Current Medical Research and Opinion |volume=24 |issue=5 |pages=1345–1357 |doi=10.1185/030079908X280707 |pmid=18384709 |quote=When oral formulations of psychostimulants are used at recommended doses and frequencies, they are unlikely to yield effects consistent with abuse potential in patients with ADHD.}}</ref> Trên thực tế, liệu pháp kích thích suốt đời đối với ADHD bắt đầu từ lúc còn nhỏ giúp giảm nguy cơ tiến triển thành mắc [[Rối loạn sử dụng chất gây nghiện|rối loạn tâm thần do sử dụng chất gây nghiện]] khi trưởng thành.<ref name="Long-Term Outcomes Medications" /> [[Con đường trung não hồi viền|Con đường trung não-hồi viền]] (''mesolimbic pathway'', hay con đường phần thưởng) là con đường dopamine kết nối [[vùng mái não giữa]] (''ventral tegmental area'', VTA) với [[nhân cạp]] (''nucleus accumbens'', NAc). Sự hoạt động quá mức bệnh lý của con đường trung não-hồi viền trên đóng một vai trò trung tâm trong nghiện amphetamin.<ref name="Amphetamine KEGG – ΔFosB">{{Chú thích web|url=http://www.genome.jp/kegg-bin/show_pathway?hsa05031|tựa đề=Amphetamine – Homo sapiens (human)|tác giả=Kanehisa Laboratories|ngày=10 October 2014|website=KEGG Pathway|ngày truy cập=31 October 2014}}</ref><ref name="Magnesium">{{Chú thích tập san học thuật |last=Nechifor M |date=March 2008 |title=Magnesium in drug dependences |url=https://www.jle.com/10.1684/mrh.2008.0124 |journal=Magnesium Research |volume=21 |issue=1 |pages=5–15 |doi=10.1684/mrh.2008.0124 |doi-broken-date=31 July 2022 |pmid=18557129}}</ref> Những người thường xuyên dùng amphetamin liều cao có nguy cơ cao bị nghiện amphetamin, vì việc sử dụng lâu dài ở liều cao dần dần làm tăng mức độ tích lũy protein ΔFosB tại nhân cạp, gây nên biểu hiện nghiện.<ref name="What the ΔFosB?" /><ref name="Nestler">{{Chú thích tập san học thuật |vauthors=Robison AJ, Nestler EJ |date=November 2011 |title=Transcriptional and epigenetic mechanisms of addiction |journal=Nature Reviews Neuroscience |volume=12 |issue=11 |pages=623–637 |doi=10.1038/nrn3111 |pmc=3272277 |pmid=21989194 |quote=ΔFosB has been linked directly to several addiction-related behaviors ... Importantly, genetic or viral overexpression of ΔJunD, a dominant negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure<sup>14,22–24</sup>. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high fat food, sex, wheel running, where it promotes that consumption<sup>14,26–30</sup>. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states. ... ΔFosB serves as one of the master control proteins governing this structural plasticity.}}</ref> Một khi nhân cạp tích lũy ΔFosB được biểu hiện quá mức, mức độ nghiêm trọng của hành vi gây nghiện sẽ tăng dần (tức là người nghiện sẽ phải tự mình tìm ma túy).<ref name="What the ΔFosB?">{{Chú thích tập san học thuật |last=Ruffle JK |date=November 2014 |title=Molecular neurobiology of addiction: what's all the (Δ)FosB about? |journal=The American Journal of Drug and Alcohol Abuse |volume=40 |issue=6 |pages=428–437 |doi=10.3109/00952990.2014.933840 |pmid=25083822 |quote=ΔFosB is an essential transcription factor implicated in the molecular and behavioral pathways of addiction following repeated drug exposure.}}</ref><ref name="Natural and drug addictions">{{Chú thích tập san học thuật |last=Olsen CM |date=December 2011 |title=Natural rewards, neuroplasticity, and non-drug addictions |journal=Neuropharmacology |volume=61 |issue=7 |pages=1109–1122 |doi=10.1016/j.neuropharm.2011.03.010 |pmc=3139704 |pmid=21459101 |quote=Similar to environmental enrichment, studies have found that exercise reduces self-administration and relapse to drugs of abuse (Cosgrove et al., 2002; Zlebnik et al., 2010). There is also some evidence that these preclinical findings translate to human populations, as exercise reduces withdrawal symptoms and relapse in abstinent smokers (Daniel et al., 2006; Prochaska et al., 2008), and one drug recovery program has seen success in participants that train for and compete in a marathon as part of the program (Butler, 2005). ... In humans, the role of dopamine signaling in incentive-sensitization processes has recently been highlighted by the observation of a dopamine dysregulation syndrome in some patients taking dopaminergic drugs. This syndrome is characterized by a medication-induced increase in (or compulsive) engagement in non-drug rewards such as gambling, shopping, or sex (Evans et al., 2006; Aiken, 2007; Lader, 2008).}}</ref> Mặc dù hiện tại không có loại thuốc hiệu quả nào để điều trị nghiện amphetamin, việc tập các bài tập hiếu khí thường xuyên, liên tục dường như có thể làm giảm nguy cơ phát triển của nghiện.<ref name="Running vs addiction">{{Chú thích tập san học thuật |vauthors=Lynch WJ, Peterson AB, Sanchez V, Abel J, Smith MA |date=September 2013 |title=Exercise as a novel treatment for drug addiction: a neurobiological and stage-dependent hypothesis |journal=Neuroscience & Biobehavioral Reviews |volume=37 |issue=8 |pages=1622–1644 |doi=10.1016/j.neubiorev.2013.06.011 |pmc=3788047 |pmid=23806439 |quote=These findings suggest that exercise may "magnitude"-dependently prevent the development of an addicted phenotype possibly by blocking/reversing behavioral and neuroadaptive changes that develop during and following extended access to the drug. ... Exercise has been proposed as a treatment for drug addiction that may reduce drug craving and risk of relapse. Although few clinical studies have investigated the efficacy of exercise for preventing relapse, the few studies that have been conducted generally report a reduction in drug craving and better treatment outcomes ... Taken together, these data suggest that the potential benefits of exercise during relapse, particularly for relapse to psychostimulants, may be mediated via chromatin remodeling and possibly lead to greater treatment outcomes.}}</ref><ref name="Exercise, addiction prevention, and ΔFosB">{{Chú thích tập san học thuật |vauthors=Zhou Y, Zhao M, Zhou C, Li R |date=July 2015 |title=Sex differences in drug addiction and response to exercise intervention: From human to animal studies |journal=Frontiers in Neuroendocrinology |volume=40 |pages=24–41 |doi=10.1016/j.yfrne.2015.07.001 |pmc=4712120 |pmid=26182835 |quote=Collectively, these findings demonstrate that exercise may serve as a substitute or competition for drug abuse by changing ΔFosB or cFos immunoreactivity in the reward system to protect against later or previous drug use. ... The postulate that exercise serves as an ideal intervention for drug addiction has been widely recognized and used in human and animal rehabilitation.}}</ref> Tập các bài tập hiếu khí thường xuyên liên tục có thể là một phương pháp điều trị hiệu quả cho người nghiện amphetamin. Liệu pháp tập thể dục cải thiện kết quả điều trị [[wiktionary:clinical|lâm sàng]] và có thể được sử dụng như một [[liệu pháp bổ trợ]] với các [[liệu pháp hành vi]] để điều trị nghiện.<ref name="Running vs addiction" /><ref name="Exercise Rev 3">{{Chú thích tập san học thuật |vauthors=Linke SE, Ussher M |date=January 2015 |title=Exercise-based treatments for substance use disorders: evidence, theory, and practicality |journal=The American Journal of Drug and Alcohol Abuse |volume=41 |issue=1 |pages=7–15 |doi=10.3109/00952990.2014.976708 |pmc=4831948 |pmid=25397661 |quote=The limited research conducted suggests that exercise may be an effective adjunctive treatment for SUDs. In contrast to the scarce intervention trials to date, a relative abundance of literature on the theoretical and practical reasons supporting the investigation of this topic has been published. ... numerous theoretical and practical reasons support exercise-based treatments for SUDs, including psychological, behavioral, neurobiological, nearly universal safety profile, and overall positive health effects.}}</ref> |
|||
==== Cơ chế phân tử sinh học ==== |
|||
Sử dụng amphetamin lâu ngày với liều lượng quá cao gây ra những thay đổi trong [[biểu hiện gen]] trong con đường trung não-hồi viền, phát sinh thông qua cơ chế [[phiên mã]] và [[di truyền học biểu sinh]].<ref name="Nestler">{{Chú thích tập san học thuật |vauthors=Robison AJ, Nestler EJ |date=November 2011 |title=Transcriptional and epigenetic mechanisms of addiction |journal=Nature Reviews Neuroscience |volume=12 |issue=11 |pages=623–637 |doi=10.1038/nrn3111 |pmc=3272277 |pmid=21989194 |quote=ΔFosB has been linked directly to several addiction-related behaviors ... Importantly, genetic or viral overexpression of ΔJunD, a dominant negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure<sup>14,22–24</sup>. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high fat food, sex, wheel running, where it promotes that consumption<sup>14,26–30</sup>. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states. ... ΔFosB serves as one of the master control proteins governing this structural plasticity.}}</ref><ref name="Nestler, Hyman, and Malenka 2">{{Chú thích tập san học thuật |vauthors=Hyman SE, Malenka RC, Nestler EJ |date=July 2006 |title=Neural mechanisms of addiction: the role of reward-related learning and memory |url=https://pdfs.semanticscholar.org/fc1e/144037cd3c08aaf32d0a92b8c55a6ae451a5.pdf |journal=Annual Review of Neuroscience |volume=29 |pages=565–598 |doi=10.1146/annurev.neuro.29.051605.113009 |pmid=16776597 |archive-url=https://web.archive.org/web/20180919115435/https://pdfs.semanticscholar.org/fc1e/144037cd3c08aaf32d0a92b8c55a6ae451a5.pdf |archive-date=2018-09-19}}</ref><ref name="Addiction genetics">{{Chú thích tập san học thuật |vauthors=Steiner H, Van Waes V |date=January 2013 |title=Addiction-related gene regulation: risks of exposure to cognitive enhancers vs. other psychostimulants |journal=Progress in Neurobiology |volume=100 |pages=60–80 |doi=10.1016/j.pneurobio.2012.10.001 |pmc=3525776 |pmid=23085425}}</ref> Các [[yếu tố phiên mã]] quan trọng nhất [note 11] tạo ra những thay đổi này là ''Delta FBJ murine osteosarcoma viral oncogene homolog B'' ([[ΔFosB]]), ''[[Cyclic adenosine monophosphate|cAMP]]'' ''response element binding protein'' ([[Protein liên kết phần tử phản ứng CAMP|CREB]], tạm dịch: ''protein gắn yếu tố đáp ứng cAMP'') và ''nuclear factor-kappa B'' ([[NF-κB]], tạm dịch: ''Yếu tố hạt nhân tăng cường chuỗi nhẹ kappa của các tế bào B hoạt động'').<ref name="Nestler" /><ref>Xem cách sử dụng thuật ngữ tại [[https://tapchiyhocvietnam.vn/index.php/vmj/article/view/54|tạp https://tapchiyhocvietnam.vn/index.php/vmj/article/view/54] Tạp chí Y học Việt Nam]</ref> ΔFosB là cơ chế phân tử sinh học quan trọng nhất trong chứng nghiện vì gen ΔFosB biểu hiện quá mức (tức là mức độ biểu hiện gen cao bất thường khi tạo ra [[kiểu hình]]) trong các neuron gai trung gian (''medium spiny neurons'') loại D1 trong [[nhân cạp]] (''nucleus accumbens'') là điều kiện [[cần và đủ]] [note 12] để có những thích ứng liên quan đến thần kinh và những sự điều chỉnh liên quan đến hành vi nghiện (ví dụ: tự tiêm chất gây nghiện theo chiều hướng tăng dần về liều).<ref name="What the ΔFosB?">{{Chú thích tập san học thuật |last=Ruffle JK |date=November 2014 |title=Molecular neurobiology of addiction: what's all the (Δ)FosB about? |journal=The American Journal of Drug and Alcohol Abuse |volume=40 |issue=6 |pages=428–437 |doi=10.3109/00952990.2014.933840 |pmid=25083822 |quote=ΔFosB is an essential transcription factor implicated in the molecular and behavioral pathways of addiction following repeated drug exposure.}}</ref><ref name="Nestler" /> Một khi ΔFosB được biểu hiện quá mức, ΔFosB gây ra trạng thái nghiện ngày càng nghiêm trọng hơn do chính những thích ứng liên quan đến thần kinh đó lại tiếp tục làm gia tăng hơn nữa sự biểu hiện quá mức của ΔFosB.<ref name="What the ΔFosB?" /> Cơ chế này có liên quan đến nghiện [[Chứng nghiện rượu|rượu]], [[cannabinoid]], [[cocain]], [[methylphenidat]], [[nicotin]], [[Thuốc giảm đau nhóm opioid|opioid]], [[phencyclidine]], [[propofol]] và [[amphetamine thay thế|amphetamin thay thế]], v..v.[source 10] |
|||
[[ΔJunD]], một yếu tố phiên mã và [[EHMT2|G9a]], một enzym [[histone methyltransferase]], đều có tác dụng chống lại chức năng của ΔFosB và ức chế sự gia tăng biểu hiện gen của ΔFosB.<ref name="Nestler">{{Chú thích tập san học thuật |vauthors=Robison AJ, Nestler EJ |date=November 2011 |title=Transcriptional and epigenetic mechanisms of addiction |journal=Nature Reviews Neuroscience |volume=12 |issue=11 |pages=623–637 |doi=10.1038/nrn3111 |pmc=3272277 |pmid=21989194 |quote=ΔFosB has been linked directly to several addiction-related behaviors ... Importantly, genetic or viral overexpression of ΔJunD, a dominant negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure<sup>14,22–24</sup>. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high fat food, sex, wheel running, where it promotes that consumption<sup>14,26–30</sup>. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states. ... ΔFosB serves as one of the master control proteins governing this structural plasticity.}}</ref><ref name="Nestler 2014 epigenetics">{{Chú thích tập san học thuật |vauthors=Nestler EJ |date=January 2014 |title=Epigenetic mechanisms of drug addiction |journal=Neuropharmacology |volume=76 Pt B |pages=259–268 |doi=10.1016/j.neuropharm.2013.04.004 |pmc=3766384 |pmid=23643695 |quote=<!-- Short-term increases in histone acetylation generally promote behavioral responses to the drugs, while sustained increases oppose cocaine's effects, based on the actions of systemic or intra-NAc administration of HDAC inhibitors. ... Genetic or pharmacological blockade of G9a in the NAc potentiates behavioral responses to cocaine and opiates, whereas increasing G9a function exerts the opposite effect (Maze et al., 2010; Sun et al., 2012a). Such drug-induced downregulation of G9a and H3K9me2 also sensitizes animals to the deleterious effects of subsequent chronic stress (Covington et al., 2011). Downregulation of G9a increases the dendritic arborization of NAc neurons, and is associated with increased expression of numerous proteins implicated in synaptic function, which directly connects altered G9a/H3K9me2 in the synaptic plasticity associated with addiction (Maze et al., 2010).<br>G9a appears to be a critical control point for epigenetic regulation in NAc, as we know it functions in two negative feedback loops. It opposes the induction of ΔFosB, a long-lasting transcription factor important for drug addiction (Robison and Nestler, 2011), while ΔFosB in turn suppresses G9a expression (Maze et al., 2010; Sun et al., 2012a). ... Also, G9a is induced in NAc upon prolonged HDAC inhibition, which explains the paradoxical attenuation of cocaine's behavioral effects seen under these conditions, as noted above (Kennedy et al., 2013). GABAA receptor subunit genes are among those that are controlled by this feedback loop. Thus, chronic cocaine, or prolonged HDAC inhibition, induces several GABAA receptor subunits in NAc, which is associated with increased frequency of inhibitory postsynaptic currents (IPSCs). In striking contrast, combined exposure to cocaine and HDAC inhibition, which triggers the induction of G9a and increased global levels of H3K9me2, leads to blockade of GABAA receptor and IPSC regulation. -->}}</ref> ΔJunD biểu hiện quá mức trong nhân cạp, phối hợp với [[vector virus]] (''viral vector'') có thể ngăn chặn hoàn toàn nhưng biến đổi liên quan đến thần kinh và hành vi được thấy trong lạm dụng chất lâu ngày (tức là những thay đổi qua trung gian là gen ΔFosB).<ref name="Nestler" /> Tương tự, hiện tượng biểu hiện quá mức gen G9a tại nhân cạp làm tăng rõ rệt quá trình [[Methyl hóa|dimethyl hóa]] nhóm lysine dư thừa tại vị trí số 9 trên protein histon H3 (tiếng Anh: ''histone 3 lysine residue 9 dimethylation'' - [[H3K9me2]], histon H3 là một protein đóng gói DNA) và ức chế sự cảm ứng của [[tính dẻo hành vi]] (''behavioral plasticity'') và [[khả biến thần kinh]] (''neuroplasticity'') qua trung gian ΔFosB do sử dụng thuốc dài ngày,[sources 11]. Sự ức chế trên xảy ra thông qua:<ref name="Nestler" /><ref name="Nestler 2014 epigenetics" /> |
|||
# Ức chế qua trung gian H3K9me2 (''H3K9me2-mediated repression'') đối với các [[yếu tố phiên mã]] gen ΔFosB |
|||
# Ức chế qua trung gian H3K9me2 đối với các mục tiêu thúc đẩy sự phiên mã của gen ΔFosB (ví dụ: enzyme cyclin-dependent kinase 5, [[CDK5]]). |
|||
ΔFosB đóng vai trò quan trọng trong việc điều chỉnh các đáp ứng hành vi đối với [[Nghiện hành vi|hành vi nghiện]], chẳng hạn như thưởng thức bữa ăn ngon, tình dục và tập thể dục.<ref name="Natural and drug addictions">{{Chú thích tập san học thuật |last=Olsen CM |date=December 2011 |title=Natural rewards, neuroplasticity, and non-drug addictions |journal=Neuropharmacology |volume=61 |issue=7 |pages=1109–1122 |doi=10.1016/j.neuropharm.2011.03.010 |pmc=3139704 |pmid=21459101 |quote=Similar to environmental enrichment, studies have found that exercise reduces self-administration and relapse to drugs of abuse (Cosgrove et al., 2002; Zlebnik et al., 2010). There is also some evidence that these preclinical findings translate to human populations, as exercise reduces withdrawal symptoms and relapse in abstinent smokers (Daniel et al., 2006; Prochaska et al., 2008), and one drug recovery program has seen success in participants that train for and compete in a marathon as part of the program (Butler, 2005). ... In humans, the role of dopamine signaling in incentive-sensitization processes has recently been highlighted by the observation of a dopamine dysregulation syndrome in some patients taking dopaminergic drugs. This syndrome is characterized by a medication-induced increase in (or compulsive) engagement in non-drug rewards such as gambling, shopping, or sex (Evans et al., 2006; Aiken, 2007; Lader, 2008).}}</ref><ref name="Nestler" /><ref name="ΔFosB reward">{{Chú thích tập san học thuật |vauthors=Blum K, Werner T, Carnes S, Carnes P, Bowirrat A, Giordano J, Oscar-Berman M, Gold M |date=March 2012 |title=Sex, drugs, and rock 'n' roll: hypothesizing common mesolimbic activation as a function of reward gene polymorphisms |journal=Journal of Psychoactive Drugs |volume=44 |issue=1 |pages=38–55 |doi=10.1080/02791072.2012.662112 |pmc=4040958 |pmid=22641964 |quote=It has been found that deltaFosB gene in the NAc is critical for reinforcing effects of sexual reward. Pitchers and colleagues (2010) reported that sexual experience was shown to cause DeltaFosB accumulation in several limbic brain regions including the NAc, medial pre-frontal cortex, VTA, caudate, and putamen, but not the medial preoptic nucleus. ... these findings support a critical role for DeltaFosB expression in the NAc in the reinforcing effects of sexual behavior and sexual experience-induced facilitation of sexual performance. ... both drug addiction and sexual addiction represent pathological forms of neuroplasticity along with the emergence of aberrant behaviors involving a cascade of neurochemical changes mainly in the brain's rewarding circuitry.}}</ref> Vì những "phần thưởng" nêu trên và thuốc gây nghiện đều gây ra [[biểu hiện gen]] của gen ΔFosB (tức là khiến não sản xuất ra nhiều hơn), việc lâu dài tiếp nhận các "phần thưởng" nêu trên cũng có thể dẫn đến tình trạng nghiện bệnh lý.<ref name="Natural and drug addictions" /><ref name="Nestler">{{Chú thích tập san học thuật |vauthors=Robison AJ, Nestler EJ |date=November 2011 |title=Transcriptional and epigenetic mechanisms of addiction |journal=Nature Reviews Neuroscience |volume=12 |issue=11 |pages=623–637 |doi=10.1038/nrn3111 |pmc=3272277 |pmid=21989194 |quote=ΔFosB has been linked directly to several addiction-related behaviors ... Importantly, genetic or viral overexpression of ΔJunD, a dominant negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure<sup>14,22–24</sup>. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high fat food, sex, wheel running, where it promotes that consumption<sup>14,26–30</sup>. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states. ... ΔFosB serves as one of the master control proteins governing this structural plasticity.}}<cite class="citation journal cs1" data-ve-ignore="true" id="CITEREFRobisonNestler2011">Robison AJ, Nestler EJ (November 2011). [//www.ncbi.nlm.nih.gov/pmc/articles/PMC3272277 "Transcriptional and epigenetic mechanisms of addiction"]. ''Nature Reviews Neuroscience''. '''12''' (11): 623–637. [[DOI|doi]]:[[doi:10.1038/nrn3111|10.1038/nrn3111]]. [[PubMed Central|PMC]] <span class="cs1-lock-free" title="Freely accessible">[//www.ncbi.nlm.nih.gov/pmc/articles/PMC3272277 3272277]</span>. [[PubMed|PMID]] [//pubmed.ncbi.nlm.nih.gov/21989194 21989194].<q>ΔFosB has been linked directly to several addiction-related behaviors ... Importantly, genetic or viral overexpression of ΔJunD, a dominant negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure<sup>14,22–24</sup>. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high fat food, sex, wheel running, where it promotes that consumption<sup>14,26–30</sup>. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states. ... ΔFosB serves as one of the master control proteins governing this structural plasticity.</q></cite></ref> Do đó, ΔFosB là yếu tố quan trọng nhất liên quan đến cả nghiện amphetamin và [[nghiện tình dục]] do amphetamin, là những hành vi tình dục cưỡng bức do hoạt động tình dục quá mức và sử dụng amphetamin.<ref name="Natural and drug addictions" /><ref name="Amph-Sex X-sensitization through D1 signaling">{{Chú thích tập san học thuật |vauthors=Pitchers KK, Vialou V, Nestler EJ, Laviolette SR, Lehman MN, Coolen LM |date=February 2013 |title=Natural and drug rewards act on common neural plasticity mechanisms with ΔFosB as a key mediator |journal=The Journal of Neuroscience |volume=33 |issue=8 |pages=3434–3442 |doi=10.1523/JNEUROSCI.4881-12.2013 |pmc=3865508 |pmid=23426671}}</ref><ref name="Amph-Sex X-sensitization through NMDA signaling">{{Chú thích tập san học thuật |vauthors=Beloate LN, Weems PW, Casey GR, Webb IC, Coolen LM |date=February 2016 |title=Nucleus accumbens NMDA receptor activation regulates amphetamine cross-sensitization and deltaFosB expression following sexual experience in male rats |journal=Neuropharmacology |volume=101 |pages=154–164 |doi=10.1016/j.neuropharm.2015.09.023 |pmid=26391065}}</ref> Những chứng nghiện tình dục này có liên quan đến [[hội chứng rối loạn điều hòa dopamin]] xảy ra ở một số bệnh nhân dùng [[Dopaminergic|thuốc dopaminergic]].<ref name="Natural and drug addictions" /><ref name="ΔFosB reward" /> |
|||
Tác dụng của amphetamin đối với sự điều hòa gen phụ thuộc vào liều lượng và đường dùng.<ref name="Addiction genetics">{{Chú thích tập san học thuật |vauthors=Steiner H, Van Waes V |date=January 2013 |title=Addiction-related gene regulation: risks of exposure to cognitive enhancers vs. other psychostimulants |journal=Progress in Neurobiology |volume=100 |pages=60–80 |doi=10.1016/j.pneurobio.2012.10.001 |pmc=3525776 |pmid=23085425}}</ref> Hầu hết các nghiên cứu về điều hòa gen và nghiện đều dựa trên các nghiên cứu trên động vật, đều là những thí nghiệm amphetamin tiêm tĩnh mạch với liều rất cao.<ref name="Addiction genetics" /> Một vài nghiên cứu đã sử dụng liều điều trị tương đương (tức là liều được điều chỉnh theo cân nặng) ở người và dùng thuốc bằng đường uống cho thấy rằng những thay đổi trong điều hòa gen là tương đối nhỏ hoặc không có.<ref name="Addiction genetics" /> Như vậy, việc sử dụng amphetamin trong y tế không ảnh hưởng đáng kể đến sự điều hòa gen.<ref name="Addiction genetics" /> |
|||
===== Dược trị liệu (Liệu pháp hóa dược) ===== |
|||
{{Tính đến|2019|12}}, chưa thấy hiệu quả của [[dược trị liệu]] (tức là điều trị dùng thuốc) cho bệnh nhân nghiện amphetamin.<ref name="NHMH_3e-Physical dependence + psychostimulant addiction treatment">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE, Holtzman DM|publisher=McGraw-Hill Medical|year=2015|isbn=9780071827706|edition=3rd|location=New York|chapter=Chapter 16: Reinforcement and Addictive Disorders|quote=Pharmacologic treatment for psychostimulant addiction is generally unsatisfactory. As previously discussed, cessation of cocaine use and the use of other psychostimulants in dependent individuals does not produce a physical withdrawal syndrome but may produce dysphoria, anhedonia, and an intense desire to reinitiate drug use.}}</ref><ref name="SystRev-Meta analysis amphetamine addiction pharmacotherapy">{{Chú thích tập san học thuật |vauthors=Chan B, Freeman M, Kondo K, Ayers C, Montgomery J, Paynter R, Kansagara D |date=December 2019 |title=Pharmacotherapy for methamphetamine/amphetamine use disorder-a systematic review and meta-analysis |journal=Addiction |volume=114 |issue=12 |pages=2122–2136 |doi=10.1111/add.14755 |pmid=31328345}}</ref><ref name="pmid24716825">{{Chú thích tập san học thuật |vauthors=Stoops WW, Rush CR |date=May 2014 |title=Combination pharmacotherapies for stimulant use disorder: a review of clinical findings and recommendations for future research |journal=Expert Review of Clinical Pharmacology |volume=7 |issue=3 |pages=363–374 |doi=10.1586/17512433.2014.909283 |pmc=4017926 |pmid=24716825 |quote=Despite concerted efforts to identify a pharmacotherapy for managing stimulant use disorders, no widely effective medications have been approved.}}</ref> Các tổng quan hệ thống từ năm 2015 và 2016 chỉ ra rằng chất đồng vận chọn lọc [[TAAR1]] rất tiềm năng trong điều trị chứng nghiện chất kích thích tâm thần;<ref name="Miller+Grandy 2016" /><ref name="TAAR1 addiction 2015" /> tuy nhiên, {{Tính đến|2016|2}}, các hợp chất có chức năng là chất chủ vận chọn lọc TAAR1 vẫn chỉ là thuốc thử nghiệm.<ref name="Miller+Grandy 2016">{{Chú thích tập san học thuật |vauthors=Grandy DK, Miller GM, Li JX |date=February 2016 |title="TAARgeting Addiction"-The Alamo Bears Witness to Another Revolution: An Overview of the Plenary Symposium of the 2015 Behavior, Biology and Chemistry Conference |journal=Drug and Alcohol Dependence |volume=159 |pages=9–16 |doi=10.1016/j.drugalcdep.2015.11.014 |pmc=4724540 |pmid=26644139 |quote=When considered together with the rapidly growing literature in the field a compelling case emerges in support of developing TAAR1-selective agonists as medications for preventing relapse to psychostimulant abuse.}}</ref><ref name="TAAR1 addiction 2015">{{Chú thích tập san học thuật |vauthors=Jing L, Li JX |date=August 2015 |title=Trace amine-associated receptor 1: A promising target for the treatment of psychostimulant addiction |journal=European Journal of Pharmacology |volume=761 |pages=345–352 |doi=10.1016/j.ejphar.2015.06.019 |pmc=4532615 |pmid=26092759 |quote=Existing data provided robust preclinical evidence supporting the development of TAAR1 agonists as potential treatment for psychostimulant abuse and addiction.}}</ref> Nghiện amphetamin phần lớn qua thông qua sự gia tăng hoạt hóa các thụ thể dopamine và các thụ thể NMDA đồng khu trú [note 13] trong nhân cạp.<ref name="Magnesium">{{Chú thích tập san học thuật |last=Nechifor M |date=March 2008 |title=Magnesium in drug dependences |url=https://www.jle.com/10.1684/mrh.2008.0124 |journal=Magnesium Research |volume=21 |issue=1 |pages=5–15 |doi=10.1684/mrh.2008.0124 |doi-broken-date=31 July 2022 |pmid=18557129}}</ref> ion [[magnesi]] ức chế các receptor NMDA bằng cách chẹn receptor của [[kênh calci]].<ref name="Magnesium" /> Một tổng quan hệ thống dựa trên thử nghiệm lên động vật khác cho thấy rằng, việc sử dụng chất kích thích tâm thần (chất gây nghiện) làm giảm đáng kể nồng độ magnesi nội bào trong não. Điều trị bổ sung magnesi [note 14] đã được chứng minh là làm giảm việc tự tiêm amphetamin ở người, nhưng đây không phải là hình thức [[đơn trị liệu]] hiệu quả cho bệnh nhân nghiện amphetamin.<ref name="Magnesium">{{Chú thích tập san học thuật |last=Nechifor M |date=March 2008 |title=Magnesium in drug dependences |url=https://www.jle.com/10.1684/mrh.2008.0124 |journal=Magnesium Research |volume=21 |issue=1 |pages=5–15 |doi=10.1684/mrh.2008.0124 |doi-broken-date=31 July 2022 |pmid=18557129}}<cite class="citation journal cs1" data-ve-ignore="true" id="CITEREFNechifor_M2008">Nechifor M (March 2008). [https://www.jle.com/10.1684/mrh.2008.0124 "Magnesium in drug dependences"]. ''Magnesium Research''. '''21''' (1): 5–15. [[DOI|doi]]:[[doi:10.1684/mrh.2008.0124|10.1684/mrh.2008.0124]] (inactive 31 July 2022). [[PubMed|PMID]] [//pubmed.ncbi.nlm.nih.gov/18557129 18557129].</cite><span class="cs1-maint citation-comment" data-ve-ignore="true"><code class="cs1-code"><nowiki>{{</nowiki>[[Bản mẫu:Chú thích tập san học thuật|cite journal]]<nowiki>}}</nowiki></code>: CS1 maint: DOI inactive as of July 2022 ([[Danh mục: Bảo trì CS1: DOI không hoạt động kể từ tháng 7 năm 2022|link]])</span> |
|||
[[Category:CS1 maint: DOI inactive as of July 2022]]</ref> |
|||
Một tổng quan hệ thống và phân tích tổng hợp từ năm 2019 đã đánh giá hiệu quả của 17 liệu pháp hóa dược khác nhau được sử dụng trong các thử nghiệm ngẫu nhiên có đối chứng đối với bệnh nhân nghiện amphetamin và methamphetamin.<ref name="SystRev-Meta analysis amphetamine addiction pharmacotherapy">{{Chú thích tập san học thuật |vauthors=Chan B, Freeman M, Kondo K, Ayers C, Montgomery J, Paynter R, Kansagara D |date=December 2019 |title=Pharmacotherapy for methamphetamine/amphetamine use disorder-a systematic review and meta-analysis |journal=Addiction |volume=114 |issue=12 |pages=2122–2136 |doi=10.1111/add.14755 |pmid=31328345}}</ref> Kết quả: chỉ tìm thấy bằng chứng mức độ thấp cho thấy methylphenidat có thể làm giảm việc người nghiện tự tiêm amphetamin hoặc methamphetamin.<ref name="SystRev-Meta analysis amphetamine addiction pharmacotherapy">{{Chú thích tập san học thuật |vauthors=Chan B, Freeman M, Kondo K, Ayers C, Montgomery J, Paynter R, Kansagara D |date=December 2019 |title=Pharmacotherapy for methamphetamine/amphetamine use disorder-a systematic review and meta-analysis |journal=Addiction |volume=114 |issue=12 |pages=2122–2136 |doi=10.1111/add.14755 |pmid=31328345}}<cite class="citation journal cs1" data-ve-ignore="true" id="CITEREFChanFreemanKondoAyers2019">Chan B, Freeman M, Kondo K, Ayers C, Montgomery J, Paynter R, Kansagara D (December 2019). "Pharmacotherapy for methamphetamine/amphetamine use disorder-a systematic review and meta-analysis". ''Addiction''. '''114''' (12): 2122–2136. [[DOI|doi]]:[[doi:10.1111/add.14755|10.1111/add.14755]]. [[PubMed|PMID]] [//pubmed.ncbi.nlm.nih.gov/31328345 31328345]. [[Semantic Scholar|S2CID]] [https://api.semanticscholar.org/CorpusID:198136436 198136436].</cite></ref> Có bằng chứng mức thấp đến trung bình về việc hầu hết các thuốc khác được sử dụng trong các thử nghiệm nêu trên là không mang lại lợi ích, bao gồm thuốc chống trầm cảm (bupropion, [[mirtazapine]], [[sertraline]]), thuốc chống loạn thần ([[aripiprazole]]), thuốc chống co giật ([[topiramate]], [[baclofen]], [[gabapentin]]), [[naltrexone]], [[varenicline]], [[citicoline]], [[ondansetron]], [[prometa]], [[riluzole]], [[atomoxetine]], dextroamphetamin và [[modafinil]].<ref name="SystRev-Meta analysis amphetamine addiction pharmacotherapy" /> |
|||
===== Liệu pháp tâm lý hành vi ===== |
|||
Một tổng quan hệ thống năm 2018 và [[Phân tích tổng hợp|phân tích tổng hợp mạng lưới]] 50 thử nghiệm liên quan đến 12 biện pháp can thiệp tâm lý xã hội khác nhau đối với chứng nghiện amphetamin, methamphetamin, cocaine cho thấy rằng [[điều trị đa mô thức]] với cả phương pháp [[quản lý dự phòng]] (''ontingency management'') và phương pháp tiếp cận củng cố cộng đồng và đào tạo gia đình (CRAFT) có hiệu quả cao nhất (tức là tỷ lệ dừng sử dụng chất) và khả năng chấp nhận cao nhất (tức là tỷ lệ tái nghiện thấp nhất).<ref name="Psychosocial interventions network meta-analysis">{{Chú thích tập san học thuật |vauthors=De Crescenzo F, Ciabattini M, D'Alò GL, De Giorgi R, Del Giovane C, Cassar C, Janiri L, Clark N, Ostacher MJ, Cipriani A |date=December 2018 |title=Comparative efficacy and acceptability of psychosocial interventions for individuals with cocaine and amphetamine addiction: A systematic review and network meta-analysis |journal=PLOS Medicine |volume=15 |issue=12 |pages=e1002715 |doi=10.1371/journal.pmed.1002715 |pmc=6306153 |pmid=30586362}}</ref> Các phương thức điều trị khác bao gồm đơn trị liệu với quản lý dự phòng hoặc phương pháp tiếp cận củng cố cộng đồng (''community reinforcement approach''), [[liệu pháp hành vi nhận thức]], [[chương trình 12 bước]],<ref>Xem nội dung Chương trình 12 bước tại: [https://www.maihuong.gov.vn/vi/chuong-trinh-phong-chong-ma-tuy/tom-tat-chuong-trinh-dieu-tri-nghien-12-buoc-hoi-phuc.html<nowiki> trang web của bệnh viện tâm thần ban ngày Mai Hương]</nowiki></ref> liệu pháp nhóm (''non-contingent reward-based therapies''), [[liệu pháp tâm động học]] (''psychodynamic therapy'') và các liệu pháp kết hợp khác.<ref name="Psychosocial interventions network meta-analysis" /> |
|||
Ngoài ra, nghiên cứu về [[tác động sinh học thần kinh của tập thể dục]] cho thấy rằng cái bài tập dùng nhiều oxy (aerobic), đặc biệt là bài tập tập luyện sức bền (ví dụ như [[Marathon|chạy marathon]]), ngăn ngừa sự phát triển của chứng nghiện ma túy và là một [[liệu pháp bổ trợ]] hiệu quả cho bệnh nhân nghiện amphetamin. Bệnh nhân tập thể dục có kết quả điều trị tốt hơn, đặc biệt là bệnh nhân nghiện chất kích thích tâm thần.<ref name="Running vs addiction">{{Chú thích tập san học thuật |vauthors=Lynch WJ, Peterson AB, Sanchez V, Abel J, Smith MA |date=September 2013 |title=Exercise as a novel treatment for drug addiction: a neurobiological and stage-dependent hypothesis |journal=Neuroscience & Biobehavioral Reviews |volume=37 |issue=8 |pages=1622–1644 |doi=10.1016/j.neubiorev.2013.06.011 |pmc=3788047 |pmid=23806439 |quote=These findings suggest that exercise may "magnitude"-dependently prevent the development of an addicted phenotype possibly by blocking/reversing behavioral and neuroadaptive changes that develop during and following extended access to the drug. ... Exercise has been proposed as a treatment for drug addiction that may reduce drug craving and risk of relapse. Although few clinical studies have investigated the efficacy of exercise for preventing relapse, the few studies that have been conducted generally report a reduction in drug craving and better treatment outcomes ... Taken together, these data suggest that the potential benefits of exercise during relapse, particularly for relapse to psychostimulants, may be mediated via chromatin remodeling and possibly lead to greater treatment outcomes.}}</ref><ref name="Exercise Rev 3">{{Chú thích tập san học thuật |vauthors=Linke SE, Ussher M |date=January 2015 |title=Exercise-based treatments for substance use disorders: evidence, theory, and practicality |journal=The American Journal of Drug and Alcohol Abuse |volume=41 |issue=1 |pages=7–15 |doi=10.3109/00952990.2014.976708 |pmc=4831948 |pmid=25397661 |quote=The limited research conducted suggests that exercise may be an effective adjunctive treatment for SUDs. In contrast to the scarce intervention trials to date, a relative abundance of literature on the theoretical and practical reasons supporting the investigation of this topic has been published. ... numerous theoretical and practical reasons support exercise-based treatments for SUDs, including psychological, behavioral, neurobiological, nearly universal safety profile, and overall positive health effects.}}</ref><ref name="Addiction review 2016">{{Chú thích tập san học thuật |vauthors=Carroll ME, Smethells JR |date=February 2016 |title=Sex Differences in Behavioral Dyscontrol: Role in Drug Addiction and Novel Treatments |journal=Frontiers in Psychiatry |volume=6 |pages=175 |doi=10.3389/fpsyt.2015.00175 |pmc=4745113 |pmid=26903885 |quote=Physical Exercise<br>There is accelerating evidence that physical exercise is a useful treatment for preventing and reducing drug addiction ... In some individuals, exercise has its own rewarding effects, and a behavioral economic interaction may occur, such that physical and social rewards of exercise can substitute for the rewarding effects of drug abuse. ... The value of this form of treatment for drug addiction in laboratory animals and humans is that exercise, if it can substitute for the rewarding effects of drugs, could be self-maintained over an extended period of time. Work to date in [laboratory animals and humans] regarding exercise as a treatment for drug addiction supports this hypothesis. ... Animal and human research on physical exercise as a treatment for stimulant addiction indicates that this is one of the most promising treatments on the horizon. |doi-access=free}}</ref> Đặc biệt, [[Thể dục aerobic|các bài thể dục aerobic]] làm hạn chế sử dụng tiêm chất kích thích, giảm nguy cơ tái nghiện và làm tăng số lượng thụ thể dopamine D<nowiki><sub id="mwA3Q">2</sub></nowiki> (DRD2) trong [[thể vân]]<ref name="Natural and drug addictions">{{Chú thích tập san học thuật |last=Olsen CM |date=December 2011 |title=Natural rewards, neuroplasticity, and non-drug addictions |journal=Neuropharmacology |volume=61 |issue=7 |pages=1109–1122 |doi=10.1016/j.neuropharm.2011.03.010 |pmc=3139704 |pmid=21459101 |quote=Similar to environmental enrichment, studies have found that exercise reduces self-administration and relapse to drugs of abuse (Cosgrove et al., 2002; Zlebnik et al., 2010). There is also some evidence that these preclinical findings translate to human populations, as exercise reduces withdrawal symptoms and relapse in abstinent smokers (Daniel et al., 2006; Prochaska et al., 2008), and one drug recovery program has seen success in participants that train for and compete in a marathon as part of the program (Butler, 2005). ... In humans, the role of dopamine signaling in incentive-sensitization processes has recently been highlighted by the observation of a dopamine dysregulation syndrome in some patients taking dopaminergic drugs. This syndrome is characterized by a medication-induced increase in (or compulsive) engagement in non-drug rewards such as gambling, shopping, or sex (Evans et al., 2006; Aiken, 2007; Lader, 2008).}}</ref><ref name="Addiction review 2016" /> (do sử dụng chất gây nghiện làm giảm số lượng DRD2 của thể vân).<ref name="Natural and drug addictions">{{Chú thích tập san học thuật |last=Olsen CM |date=December 2011 |title=Natural rewards, neuroplasticity, and non-drug addictions |journal=Neuropharmacology |volume=61 |issue=7 |pages=1109–1122 |doi=10.1016/j.neuropharm.2011.03.010 |pmc=3139704 |pmid=21459101 |quote=Similar to environmental enrichment, studies have found that exercise reduces self-administration and relapse to drugs of abuse (Cosgrove et al., 2002; Zlebnik et al., 2010). There is also some evidence that these preclinical findings translate to human populations, as exercise reduces withdrawal symptoms and relapse in abstinent smokers (Daniel et al., 2006; Prochaska et al., 2008), and one drug recovery program has seen success in participants that train for and compete in a marathon as part of the program (Butler, 2005). ... In humans, the role of dopamine signaling in incentive-sensitization processes has recently been highlighted by the observation of a dopamine dysregulation syndrome in some patients taking dopaminergic drugs. This syndrome is characterized by a medication-induced increase in (or compulsive) engagement in non-drug rewards such as gambling, shopping, or sex (Evans et al., 2006; Aiken, 2007; Lader, 2008).}}<cite class="citation journal cs1" data-ve-ignore="true" id="CITEREFOlsen_CM2011">Olsen CM (December 2011). [//www.ncbi.nlm.nih.gov/pmc/articles/PMC3139704 "Natural rewards, neuroplasticity, and non-drug addictions"]. ''Neuropharmacology''. '''61''' (7): 1109–1122. [[DOI|doi]]:[[doi:10.1016/j.neuropharm.2011.03.010|10.1016/j.neuropharm.2011.03.010]]. [[PubMed Central|PMC]] <span class="cs1-lock-free" title="Freely accessible">[//www.ncbi.nlm.nih.gov/pmc/articles/PMC3139704 3139704]</span>. [[PubMed|PMID]] [//pubmed.ncbi.nlm.nih.gov/21459101 21459101].<q>Similar to environmental enrichment, studies have found that exercise reduces self-administration and relapse to drugs of abuse (Cosgrove et al., 2002; Zlebnik et al., 2010). There is also some evidence that these preclinical findings translate to human populations, as exercise reduces withdrawal symptoms and relapse in abstinent smokers (Daniel et al., 2006; Prochaska et al., 2008), and one drug recovery program has seen success in participants that train for and compete in a marathon as part of the program (Butler, 2005). ... In humans, the role of dopamine signaling in incentive-sensitization processes has recently been highlighted by the observation of a dopamine dysregulation syndrome in some patients taking dopaminergic drugs. This syndrome is characterized by a medication-induced increase in (or compulsive) engagement in non-drug rewards such as gambling, shopping, or sex (Evans et al., 2006; Aiken, 2007; Lader, 2008).</q></cite></ref> Một nghiên cứu cho thấy rằng tập thể dục cũng có thể ngăn ngừa sự phát triển của hành vi nghiện ma túy bằng cách thay đổi hoạt tính miễn dịch ΔFosB hoặc {{Nowrap|[[c-Fos]]}} trong thể vân hoặc các vùng khác của [[hệ thống phần thưởng]].<ref name="Exercise, addiction prevention, and ΔFosB">{{Chú thích tập san học thuật |vauthors=Zhou Y, Zhao M, Zhou C, Li R |date=July 2015 |title=Sex differences in drug addiction and response to exercise intervention: From human to animal studies |journal=Frontiers in Neuroendocrinology |volume=40 |pages=24–41 |doi=10.1016/j.yfrne.2015.07.001 |pmc=4712120 |pmid=26182835 |quote=Collectively, these findings demonstrate that exercise may serve as a substitute or competition for drug abuse by changing ΔFosB or cFos immunoreactivity in the reward system to protect against later or previous drug use. ... The postulate that exercise serves as an ideal intervention for drug addiction has been widely recognized and used in human and animal rehabilitation.}}</ref>{{FOSB addiction table|Table title=Summary of addiction-related plasticity}} |
|||
==== Sự lệ thuộc vào chất gây nghiện và hội chứng cai ==== |
|||
Khả năng [[dung nạp thuốc]] tăng lên nhanh chóng khi lạm dụng amphetamin (tức là sử dụng amphetamin để giải trí). Hệ quả, thời gian lạm dụng thuốc kéo dài khiến người nghiện phải tăng liều thuốc ngày càng cao để đạt được tác dụng tương tự.<ref name="Cochrane 2013 treatments">{{Chú thích tập san học thuật |vauthors=Perez-Mana C, Castells X, Torrens M, Capella D, Farre M |date=September 2013 |title=Efficacy of psychostimulant drugs for amphetamine abuse or dependence |journal=Cochrane Database of Systematic Reviews |volume=9 |issue=9 |pages=CD009695 |doi=10.1002/14651858.CD009695.pub2 |pmid=23996457}}</ref><ref>{{Chú thích web|url=http://www.merckmanuals.com/home/special_subjects/drug_use_and_abuse/amphetamines.html|tựa đề=Amphetamines: Drug Use and Abuse|ngày=February 2003|website=Merck Manual Home Edition|nhà xuất bản=Merck|url lưu trữ=https://web.archive.org/web/20070217053619/http://www.merck.com/mmhe/sec07/ch108/ch108g.html|ngày lưu trữ=17 February 2007|ngày truy cập=28 February 2007}}</ref> Theo một tổng quan hệ thống của tổ chức Cochrane về việc [[cai nghiện]] ở những người sử dụng amphetamin và methamphetamin, "khi người dùng liều cao, lâu dài chất gây nghiện bỗng dưng đột ngột ngừng sử dụng amphetamin, [[hội chứng cai]] xảy ra trong vòng 24 giờ kể từ liều dùng thuốc cuối cùng. "<ref name="Cochrane Withdrawal">{{Chú thích tập san học thuật |vauthors=Shoptaw SJ, Kao U, Heinzerling K, Ling W |date=April 2009 |title=Treatment for amphetamine withdrawal |journal=Cochrane Database of Systematic Reviews |issue=2 |pages=CD003021 |doi=10.1002/14651858.CD003021.pub2 |pmc=7138250 |pmid=19370579 |quote=The prevalence of this withdrawal syndrome is extremely common (Cantwell 1998; Gossop 1982) with 87.6% of 647 individuals with amphetamine dependence reporting six or more signs of amphetamine withdrawal listed in the DSM when the drug is not available (Schuckit 1999) ... The severity of withdrawal symptoms is greater in amphetamine dependent individuals who are older and who have more extensive amphetamine use disorders (McGregor 2005). Withdrawal symptoms typically present within 24 hours of the last use of amphetamine, with a withdrawal syndrome involving two general phases that can last 3 weeks or more. The first phase of this syndrome is the initial "crash" that resolves within about a week (Gossop 1982;McGregor 2005) ...}}</ref> Tổng quan này lưu ý rằng hội chứng cai ở những người dùng liều cao, dùng lâu dài xảy ra thường xuyên, khoảng 88% trường hợp và kéo dài trong {{Nowrap|3–4}} tuần.<ref name="Cochrane Withdrawal" /> Hội chứng cai amphetamin gồm các triệu chứng: lo lắng, thèm ma túy, [[khí sắc trầm]], [[mệt mỏi]], [[tăng thèm ăn]], tăng hoặc giảm vận động, thiếu động lực, khó ngủ hoặc buồn ngủ, và [[giấc mơ sáng suốt]].<ref name="Cochrane Withdrawal" /> Tổng quan hệ thống chỉ ra rằng mức độ nghiêm trọng của các triệu chứng trong hội chứng cai có tương quan thuận với tuổi và mức độ phụ thuộc của từng người.<ref name="Cochrane Withdrawal" /> Ngừng điều trị bằng amphetamin ở liều điều trị gây các triệu chứng cai mức độ nhẹ, có thể tránh hội chứng cai bằng cách giảm liều từ từ.<ref name="Stahl's Essential Psychopharmacology">{{Chú thích sách|title=Prescriber's Guide: Stahl's Essential Psychopharmacology|vauthors=Stahl SM|date=March 2017|publisher=Cambridge University Press|isbn=9781108228749|edition=6th|location=Cambridge, United Kingdom|pages=45–51|chapter=Amphetamine (D,L)|access-date=5 August 2017|chapter-url=https://books.google.com/books?id=9hssDwAAQBAJ&pg=PA45}}</ref> |
|||
== Quá liều == |
|||
Quá liều amphetamin dẫn đến nhiều triệu chứng khác nhau, nhưng hiếm khi gây tử vong nếu được chăm sóc kịp thời.<ref name="Stahl's Essential Psychopharmacology">{{Chú thích sách|title=Prescriber's Guide: Stahl's Essential Psychopharmacology|vauthors=Stahl SM|date=March 2017|publisher=Cambridge University Press|isbn=9781108228749|edition=6th|location=Cambridge, United Kingdom|pages=45–51|chapter=Amphetamine (D,L)|access-date=5 August 2017|chapter-url=https://books.google.com/books?id=9hssDwAAQBAJ&pg=PA45}}</ref><ref name="Amphetamine toxidrome">{{Chú thích tập san học thuật |vauthors=Spiller HA, Hays HL, Aleguas A |date=June 2013 |title=Overdose of drugs for attention-deficit hyperactivity disorder: clinical presentation, mechanisms of toxicity, and management |journal=CNS Drugs |volume=27 |issue=7 |pages=531–543 |doi=10.1007/s40263-013-0084-8 |pmid=23757186 |quote=Amphetamine, dextroamphetamine, and methylphenidate act as substrates for the cellular monoamine transporter, especially the dopamine transporter (DAT) and less so the norepinephrine (NET) and serotonin transporter. The mechanism of toxicity is primarily related to excessive extracellular dopamine, norepinephrine, and serotonin.}}</ref> Mức độ nghiêm trọng của các triệu chứng quá liều tăng theo liều lượng và giảm khi có sự dung nạp thuốc với amphetamin.<ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref> Người nghiện có sự lệ thuộc cơ thể vào thuốc có thể dùng tới 5 gam amphetamin trong một ngày, khoảng 100 lần liều điều trị tối đa hàng ngày. Các triệu chứng của quá liều vừa phải và nặng được liệt kê ở bảng dưới đây. Ngộ độc amphetamin gây tử vong có triệu chứng co giật và [[hôn mê]].<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref name="Westfall" /> Năm 2013, sử dụng quá liều amphetamin, methamphetamin và các hợp chất khác có liên quan đến " [[Phụ thuộc amphetamine|rối loạn sử dụng amphetamin]] ", khiến 3788 số ca tử vong trên toàn thế giới ({{Nowrap|3425–4145}} tử vong, [[Khoảng tin cậy|khoảng tin cậy 95%]]). [note 15]<ref name="GDB2013">{{Chú thích tập san học thuật |vauthors=Collaborators |year=2015 |title=Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013 |url= |journal=The Lancet |volume=385 |issue=9963 |pages=117–171 |doi=10.1016/S0140-6736(14)61682-2 |pmc=4340604 |pmid=25530442 |quote=Amphetamine use disorders ... 3,788 (3,425–4,145)}}</ref> |
|||
{| class="wikitable center" style="margin: 1em auto;" |
|||
|+Các triệu chứng quá liều theo hệ cơ quan |
|||
! scope="col" style="text-align:center" | Hệ cơ quan |
|||
! scope="col" style="width: 40%;" | Quá liều nhẹ hoặc vừa phải<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref> |
|||
! scope="col" style="width: 50%;" | Quá liều nặng |
|||
|- |
|||
! scope="row" | [[Hệ tuần hoàn|Tim mạch]] |
|||
| |
|||
* [[Rối loạn nhịp tim]] |
|||
* [[tăng huyết áp]] hoặc [[Huyết áp thấp|tụt huyết áp]] |
|||
| |
|||
* [[Sốc tim]] (tim không bơm đủ máu) |
|||
* [[Xuất huyết não]] (chảy máu não) |
|||
* [[Trụy tuần hoàn]] (suy một phần hoặc hoàn toàn [[hệ tuần hoàn]]) |
|||
|- |
|||
! scope="row" | [[Hệ thần kinh trung ương|Hệ thần kinh trung ương<br /><br /><br />]] |
|||
| |
|||
* Hoang mang |
|||
* Tăng phản xạ |
|||
* Kích động nặng |
|||
* [[Run]] (co giật cơ không tự chủ) |
|||
| |
|||
* [[Rối loạn tâm thần do chất kích thích|Rối loạn tâm thần do amphetamin cấp]] (ví dụ, [[hoang tưởng]] và [[Hoang tưởng ảo giác|paranoid]]) |
|||
* [[Hành vi rập khuôn]], máy móc |
|||
* [[Hội chứng serotonin]] |
|||
* [[Bão adrenergic]] |
|||
|- |
|||
! scope="row" | [[Hệ vận động|Cơ xương khớp]] |
|||
| |
|||
* [[Đau cơ]] |
|||
| |
|||
* [[Tiêu cơ vân]] (phân hủy cơ) |
|||
|- |
|||
! scope="row" | [[Hệ hô hấp|Hô hấp]] |
|||
| |
|||
* Thở nhanh |
|||
| |
|||
* [[Phù phổi]] (tích tụ dịch trong phổi) |
|||
* [[Tăng huyết áp phổi|Tăng áp phổi]] (tăng huyết áp [[động mạch phổi]]) |
|||
* [[Kiềm hô hấp]] (giảm nồng độ [[Carbon dioxide|CO<sub>2</sub>]] trong máu) |
|||
|- |
|||
! scope="row" | Tiết niệu |
|||
| |
|||
* [[Đái buốt]] |
|||
* [[Bí tiểu]] |
|||
| |
|||
* [[Vô niệu]] |
|||
* [[Suy thận]] |
|||
|- |
|||
! scope="row" | Khác |
|||
| |
|||
* [[Tăng thân nhiệt]] |
|||
* [[Giãn đồng tử|Giãn]] đồng tử |
|||
| |
|||
* [[Tăng kali máu|Tăng]] hoặc [[hạ kali máu]] |
|||
* [[Tăng thân nhiệt ác tính]] |
|||
* [[Nhiễm toan chuyển hóa|Toan chuyển hóa]] |
|||
|} |
|||
=== Độc tính === |
|||
Ở động vật gặm nhấm và động vật linh trưởng, amphetamin liều đủ cao gây ra [[độc tính thần kinh]] dopaminergic, hoặc làm tổn thương neuron dopamine. Tổn thương này đặc trưng bởi sự [[Thoái hóa thần kinh|thoái hóa]] đuôi sợi trục neuron dopamine và giảm chức năng vận chuyển và thụ thể.<ref name="Humans&Animals">{{Chú thích tập san học thuật |last=Advokat C |date=July 2007 |title=Update on amphetamine neurotoxicity and its relevance to the treatment of ADHD |journal=Journal of Attention Disorders |volume=11 |issue=1 |pages=8–16 |doi=10.1177/1087054706295605 |pmid=17606768}}</ref><ref name="Amph-induced hyperthermia and neurotoxicity review" /> Không có bằng chứng cho thấy amphetamin gây độc trực tiếp cho thần kinh ở người.<ref>{{Chú thích web|url=http://toxnet.nlm.nih.gov/cgi-bin/sis/search/r?dbs+hsdb:@term+@rn+@rel+300-62-9|tựa đề=Amphetamine|website=United States National Library of Medicine – Toxicology Data Network|nhà xuất bản=Hazardous Substances Data Bank|url lưu trữ=https://web.archive.org/web/20171002194327/https://toxnet.nlm.nih.gov/cgi-bin/sis/search2/cgi-bin/sis/search2/f?.%2Ftemp%2F~mdjW95%3A1%3AFULL|ngày lưu trữ=2 October 2017|ngày truy cập=2 October 2017|trích dẫn=Direct toxic damage to vessels seems unlikely because of the dilution that occurs before the drug reaches the cerebral circulation.}}</ref><ref name="Malenka_2009_02">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE|publisher=McGraw-Hill Medical|year=2009|isbn=9780071481274|veditors=Sydor A, Brown RY|edition=2nd|location=New York, USA|page=370|chapter=Chapter 15: Reinforcement and addictive disorders|quote=Unlike cocaine and amphetamine, methamphetamine is directly toxic to midbrain dopamine neurons.}}</ref> Tuy nhiên, dùng amphetamin với liều lớn có thể gián tiếp gây ra độc tính thần kinh dopaminergic do [[tăng thân nhiệt ác tính]], hình thành quá mức các [[loài oxy phản ứng]] (''reactive oxygen species'' - ROS)<ref>Thuật ngữ lấy từ<nowiki>[http://hoithankinhhocvietnam.com.vn/tham-luan-ve-goc-tu-do/ Tham luận về gốc tự do của Hội Thần kinh học Việt Nam]</nowiki></ref> và tăng quá trình [[tự oxy hóa]] (''autoxidation'') dopamine. Các mô hình động vật về ngộ độc thần kinh do tiếp xúc với amphetamin liều cao cho thấy sự xuất hiện của tăng thân nhiệt ác tính (tức là [[Nhiệt độ cơ thể con người|nhiệt độ cơ thể]] ≥ 40 ° C) cần thiết cho quá trình tiến triển ngộ độc thần kinh do amphetamin.<ref name="Amph-induced hyperthermia and neurotoxicity review">{{Chú thích tập san học thuật |vauthors=Bowyer JF, Hanig JP |date=November 2014 |title=Amphetamine- and methamphetamine-induced hyperthermia: Implications of the effects produced in brain vasculature and peripheral organs to forebrain neurotoxicity |journal=Temperature |volume=1 |issue=3 |pages=172–182 |doi=10.4161/23328940.2014.982049 |pmc=5008711 |pmid=27626044 |quote=Hyperthermia alone does not produce amphetamine-like neurotoxicity but AMPH and METH exposures that do not produce hyperthermia (≥40 °C) are minimally neurotoxic. Hyperthermia likely enhances AMPH and METH neurotoxicity directly through disruption of protein function, ion channels and enhanced ROS production. ... The hyperthermia and the hypertension produced by high doses amphetamines are a primary cause of transient breakdowns in the blood-brain barrier (BBB) resulting in concomitant regional neurodegeneration and neuroinflammation in laboratory animals. ... In animal models that evaluate the neurotoxicity of AMPH and METH, it is quite clear that hyperthermia is one of the essential components necessary for the production of histological signs of dopamine terminal damage and neurodegeneration in cortex, striatum, thalamus and hippocampus.}}</ref> Nhiệt độ não tăng trên 40 ° C kéo dài có thể thúc đẩy sự phát triển của độc tính thần kinh do amphetamin ở động vật thí nghiệm bằng cách tạo ra các loại oxy phản ứng, phá vỡ chức năng protein tế bào và tăng tính thấm của [[hàng rào máu não]].<ref name="Amph-induced hyperthermia and neurotoxicity review" /> |
|||
=== Rối loạn tâm thần === |
|||
Quá liều amphetamin có thể dẫn đến rối loạn tâm thần do sử dụng chất. Các triệu chứng: hoang tưởng và rối loạn hoang tưởng paranoid.<ref name="Cochrane2">{{cite journal|vauthors=Shoptaw SJ, Kao U, Ling W|date=January 2009|title=Treatment for amphetamine psychosis|journal=Cochrane Database of Systematic Reviews|issue=1|pages=CD003026|doi=10.1002/14651858.CD003026.pub3|pmc=7004251|pmid=19160215|quote=A minority of individuals who use amphetamines develop full-blown psychosis requiring care at emergency departments or psychiatric hospitals. In such cases, symptoms of amphetamine psychosis commonly include paranoid and persecutory delusions as well as auditory and visual hallucinations in the presence of extreme agitation. More common (about 18%) is for frequent amphetamine users to report psychotic symptoms that are sub-clinical and that do not require high-intensity intervention ...<br />About 5–15% of the users who develop an amphetamine psychosis fail to recover completely (Hofmann 1983) ...<br />Findings from one trial indicate use of antipsychotic medications effectively resolves symptoms of acute amphetamine psychosis.<br />psychotic symptoms of individuals with amphetamine psychosis may be due exclusively to heavy use of the drug or heavy use of the drug may exacerbate an underlying vulnerability to schizophrenia.|editor=<!--Shoptaw SJ--> Shoptaw SJ, Ali R}}</ref><ref name="Amphetamine-induced psychosis">{{Chú thích tập san học thuật |vauthors=Bramness JG, Gundersen ØH, Guterstam J, Rognli EB, Konstenius M, Løberg EM, Medhus S, Tanum L, Franck J |date=December 2012 |title=Amphetamine-induced psychosis—a separate diagnostic entity or primary psychosis triggered in the vulnerable? |journal=BMC Psychiatry |volume=12 |pages=221 |doi=10.1186/1471-244X-12-221 |pmc=3554477 |pmid=23216941 |quote=In these studies, amphetamine was given in consecutively higher doses until psychosis was precipitated, often after 100–300 mg of amphetamine ... Secondly, psychosis has been viewed as an adverse event, although rare, in children with ADHD who have been treated with amphetamine}}</ref> Một tổng quan hệ thống của tổ chức Cochrane về điều trị rối loạn tâm thần bằng amphetamin, dextroamphetamin và methamphetamin cho thấy khoảng {{Nowrap|5–15%}} người nghiện không thể khỏi hoàn toàn.<ref name="Hofmann">{{Chú thích sách|url=https://archive.org/details/handbookondrugal0002hofm/page/329|title=A Handbook on Drug and Alcohol Abuse: The Biomedical Aspects|last=Hofmann FG|publisher=Oxford University Press|year=1983|isbn=9780195030570|edition=2nd|location=New York, USA|page=[https://archive.org/details/handbookondrugal0002hofm/page/329 329]}}</ref> Theo tổng quan, có ít nhất một thử nghiệm cho thấy [[thuốc chống loạn thần]] giải quyết hiệu quả các triệu chứng của rối loạn tâm thần do sử dụng amphetamin cấp tính. Rối loạn tâm thần hiếm khi phát sinh từ việc sử dụng các liệu pháp chữa trị.<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref name="Amphetamine-induced psychosis" /><ref name="Stimulant Misuse">{{Chú thích web|url=http://www.acha.org/prof_dev/ADHD_docs/ADHD_PDprogram_Article2.pdf|tựa đề=Stimulant Misuse: Strategies to Manage a Growing Problem|tác giả=Greydanus D|website=American College Health Association|nhà xuất bản=ACHA Professional Development Program|trang=20|kiểu=Review Article|url lưu trữ=https://web.archive.org/web/20131103155156/http://www.acha.org/prof_dev/ADHD_docs/ADHD_PDprogram_Article2.pdf|ngày lưu trữ=3 November 2013|ngày truy cập=2 November 2013}}</ref> |
|||
== Tương tác thuốc == |
|||
Nhiều loại dược chất được biết là có [[Tương tác thuốc|tương tác]] với amphetamin, dẫn đến tác dụng và/hoặc chuyển hóa của thuốc bị thay đổi.<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref> [[Chất ức chế enzym]] chuyển hóa amphetamin (ví dụ, [[CYP2D6]] và [[Monooxygenase 3 chứa flavin|FMO3]]) kéo dài [[thời gian bán thải]] của amphetamin, có nghĩa là tác dụng của chất sẽ kéo dài hơn.<ref name="FDA" /> Amphetamin cũng tương tác với {{Abbr|MAOIs|monoamine oxidase inhibitors}}, đặc biệt là chất ức chế [[monoamine oxidase A]], vì cả MAOI và amphetamin đều làm tăng catecholamine [[Huyết tương|trong huyết tương]] (tức là noradrenalin và dopamine);<ref name="FDA" /> do đó, việc sử dụng đồng thời cả hai chất rất nguy hiểm.<ref name="FDA" /> Amphetamin làm thay đổi tác dụng của hầu hết các loại thuốc thần kinh. Đặc biệt, amphetamin có thể làm giảm tác dụng của [[thuốc an thần]] và [[Thuốc ức chế trung ương|thuốc ức chế thần kinh]], đồng thời làm tăng tác dụng của [[Chất kích thích|thuốc kích thần]] và [[thuốc chống trầm cảm]].<ref name="FDA" /> Amphetamin cũng có thể làm giảm tác dụng của [[thuốc hạ huyết áp]] và [[thuốc chống loạn thần]] do tác dụng của chất lên huyết áp và dopamine.<ref name="FDA" /> [[Thiếu kẽm|Bổ sung kẽm]] có thể làm giảm [[Liều có hiệu quả|liều có hiệu quả tối thiểu]] (ED) của amphetamin trong điều trị ADHD.<ref name="Zinc and PEA">{{Chú thích tập san học thuật |vauthors=Scassellati C, Bonvicini C, Faraone SV, Gennarelli M |date=October 2012 |title=Biomarkers and attention-deficit/hyperactivity disorder: a systematic review and meta-analyses |journal=Journal of the American Academy of Child & Adolescent Psychiatry |volume=51 |issue=10 |pages=1003–1019.e20 |doi=10.1016/j.jaac.2012.08.015 |pmid=23021477 |quote=With regard to zinc supplementation, a placebo controlled trial reported that doses up to 30 mg/day of zinc were safe for at least 8 weeks, but the clinical effect was equivocal except for the finding of a 37% reduction in amphetamine optimal dose with 30 mg per day of zinc.<sup>110</sup>}}</ref> |
|||
Không có tương tác đáng kể khi dùng amphetamin với thức ăn, nhưng [[PH|độ pH]] của đường tiêu hóa và nước tiểu ảnh hưởng đến sự hấp thu và [[bài tiết]] của amphetamin, tương ứng.<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref> Các chất có tính acid làm giảm hấp thu amphetamin và tăng bài tiết qua nước tiểu, còn các chất có tính kiềm thì ngược lại.<ref name="FDA" /> Do ảnh hưởng của pH đối với sự hấp thụ, amphetamin cũng tương tác với thuốc làm giảm độ acid dịch vị dạ dày như [[thuốc ức chế bơm proton]] và [[Thuốc kháng histamin H2|thuốc kháng histamine H<sub>2</sub>]], làm tăng pH đường tiêu hóa (tức là kiềm hơn).<ref name="FDA" /> |
|||
== Dược học == |
|||
=== Dược lực học === |
|||
{{Amphetamine pharmacodynamics}}{{Amphetamine pharmacodynamics}}Amphetamin phát huy tác dụng bằng cách sử dụng chất dẫn truyền thần kinh [[Monoamines|monoamin]] làm tín hiệu thần kinh trong não, chủ yếu ở tế bào thần kinh [[catecholamin]] trong con đường điều hành chức năng (''executive function pathway'') và và con đường khen thưởng (''reward pathway'') của não.<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref><ref name="cognition enhancers">{{Chú thích tập san học thuật |vauthors=Bidwell LC, McClernon FJ, Kollins SH |date=August 2011 |title=Cognitive enhancers for the treatment of ADHD |journal=Pharmacology Biochemistry and Behavior |volume=99 |issue=2 |pages=262–274 |doi=10.1016/j.pbb.2011.05.002 |pmc=3353150 |pmid=21596055}}</ref> Nồng độ của các chất dẫn truyền thần kinh (dopamine và noradrenalin) có liên quan đến con đường điều hành chức năng và phần thưởng dopamine và noradrenalin. Nồng độ các chất này tăng đột ngột, phụ thuộc vào liều lượng của amphetamin vì tác dụng của amphetamin đối với các chất vận chuyển monoamin.<ref name="Miller" /><ref name="cognition enhancers" /><ref name="E Weihe">{{Chú thích tập san học thuật |vauthors=Eiden LE, Weihe E |date=January 2011 |title=VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse |journal=Annals of the New York Academy of Sciences |volume=1216 |issue=1 |pages=86–98 |bibcode=<!-- No --> |doi=10.1111/j.1749-6632.2010.05906.x |pmc=4183197 |pmid=21272013 |quote=VMAT2 is the CNS vesicular transporter for not only the biogenic amines DA, NE, EPI, 5-HT, and HIS, but likely also for the trace amines TYR, PEA, and thyronamine (THYR) ... [Trace aminergic] neurons in mammalian CNS would be identifiable as neurons expressing VMAT2 for storage, and the biosynthetic enzyme aromatic amino acid decarboxylase (AADC). ... AMPH release of DA from synapses requires both an action at VMAT2 to release DA to the cytoplasm and a concerted release of DA from the cytoplasm via "reverse transport" through DAT.}}</ref> Các tác dụng tăng cường và thúc đẩy động lực của amphetamin chủ yếu là do tăng cường hoạt động dopaminergic trong con đường trung não-hồi viền.<ref name="Malenka_2009">{{Chú thích sách|title=Molecular Neuropharmacology: A Foundation for Clinical Neuroscience|vauthors=Malenka RC, Nestler EJ, Hyman SE|publisher=McGraw-Hill Medical|year=2009|isbn=9780071481274|veditors=Sydor A, Brown RY|edition=2nd|location=New York, USA|pages=318, 321|chapter=Chapter 13: Higher Cognitive Function and Behavioral Control|quote=Therapeutic (relatively low) doses of psychostimulants, such as methylphenidate and amphetamine, improve performance on working memory tasks both in normal subjects and those with ADHD. ... stimulants act not only on working memory function, but also on general levels of arousal and, within the nucleus accumbens, improve the saliency of tasks. Thus, stimulants improve performance on effortful but tedious tasks ... through indirect stimulation of dopamine and norepinephrine receptors. ...<br>Beyond these general permissive effects, dopamine (acting via D1 receptors) and norepinephrine (acting at several receptors) can, at optimal levels, enhance working memory and aspects of attention.}}</ref> Tác dụng [[hưng phấn]] và kích thích vận động của amphetamin phụ thuộc vào cường độ và tốc độ bằng cách tăng nồng độ dopamine và noradrenalin ở synap trong [[thể vân]].<ref name="Amph Uses">{{Chú thích tập san học thuật |vauthors=Heal DJ, Smith SL, Gosden J, Nutt DJ |date=June 2013 |title=Amphetamine, past and present – a pharmacological and clinical perspective |journal=Journal of Psychopharmacology |volume=27 |issue=6 |pages=479–496 |doi=10.1177/0269881113482532 |pmc=3666194 |pmid=23539642 |quote=The intravenous use of d-amphetamine and other stimulants still pose major safety risks to the individuals indulging in this practice. Some of this intravenous abuse is derived from the diversion of ampoules of d-amphetamine, which are still occasionally prescribed in the UK for the control of severe narcolepsy and other disorders of excessive sedation. ... For these reasons, observations of dependence and abuse of prescription d-amphetamine are rare in clinical practice, and this stimulant can even be prescribed to people with a history of drug abuse provided certain controls, such as daily pick-ups of prescriptions, are put in place (Jasinski and Krishnan, 2009b).}}</ref> |
|||
Năm 2001, amphetamin được chứng minh chất chủ vận mạnh của [[TAAR1|''trace amine-associated receptor 1'']] (TAAR1), một [[Thụ thể bắt cặp với G protein|thụ thể bắt cặp với protein G]] (GPCR) ở đây là protein G<sub>s</sub> và G<sub>q</sub>. Phát hiện này rất quan trọng trong việc điều hòa các monoamine trong não..<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref><ref name="TAAR1 IUPHAR">{{Chú thích web|url=http://www.iuphar-db.org/DATABASE/ObjectDisplayForward?objectId=364|tựa đề=TA<sub>1</sub> receptor|ngày=2 December 2014|website=IUPHAR database|nhà xuất bản=International Union of Basic and Clinical Pharmacology|ngày truy cập=8 December 2014|trích dẫn=<!-- Comments: Tyramine causes an increase in intracellular cAMP in HEK293 or COS-7 cells expressing the TA1 receptor in vitro [4,6,18]. In addition, coupling to a promiscuous Gαq has been observed, resulting in increased intracellular calcium concentration [24]. -->}}</ref> Kích hoạt {{Abbr|TAAR1|trace amine-associated receptor 1}} làm tăng sản xuất {{Abbrlink|cAMP|cyclic adenosine monophosphate}} thông qua hoạt hóa [[Adenylat cyclase|adenylyl cyclase]] và ức chế chức năng [[vận chuyển monoamin]].<ref name="Miller" /><ref name="pmid11459929">{{Chú thích tập san học thuật |vauthors=Borowsky B, Adham N, Jones KA, Raddatz R, Artymyshyn R, Ogozalek KL, Durkin MM, Lakhlani PP, Bonini JA, Pathirana S, Boyle N, Pu X, Kouranova E, Lichtblau H, Ochoa FY, Branchek TA, Gerald C |date=July 2001 |title=Trace amines: identification of a family of mammalian G protein-coupled receptors |journal=Proceedings of the National Academy of Sciences |volume=98 |issue=16 |pages=8966–8971 |bibcode=2001PNAS...98.8966B |doi=10.1073/pnas.151105198 |pmc=55357 |pmid=11459929 |doi-access=free}}</ref> Các [[autoreceptor]] monoamine (ví dụ, [[D2sh|receptor dopamin D<sub>2</sub>]], [[Thụ thể adrenergic alpha-2|receptor α<sub>2</sub>]]-adrenergic, và [[5-HT1A|receptor 5-HT<sub>1</sub>]]) có tác dụng ngược lại với TAAR1, và khi các receptor (thụ thể) này phối hợp phối hợp với nhau sẽ điều hòa cho quá trình vận chuyển các monoamine.<ref name="Miller" /><ref name="Miller+Grandy 2016">{{Chú thích tập san học thuật |vauthors=Grandy DK, Miller GM, Li JX |date=February 2016 |title="TAARgeting Addiction"-The Alamo Bears Witness to Another Revolution: An Overview of the Plenary Symposium of the 2015 Behavior, Biology and Chemistry Conference |journal=Drug and Alcohol Dependence |volume=159 |pages=9–16 |doi=10.1016/j.drugalcdep.2015.11.014 |pmc=4724540 |pmid=26644139 |quote=When considered together with the rapidly growing literature in the field a compelling case emerges in support of developing TAAR1-selective agonists as medications for preventing relapse to psychostimulant abuse.}}</ref> Đặc biệt, amphetamin và các trace amin có ái lực liên kết cao đối với TAAR1, nhưng không có ái lực liên kết đối với các autoreceptor monoamine.<ref name="Miller" /><ref name="Miller+Grandy 2016" /> Các nghiên cứu hình ảnh học chỉ ra rằng amphetamin và trace amin ức chế quá trình tái hấp thu monoamine tùy vị trí đặc trưng và phụ thuộc vào có hay không sự có mặt của TAAR1 trong các tế bào thần kinh monoamin.<ref name="Miller" /> |
|||
Ngoài việc ức chế các protein vận chuyển monoamin, amphetamin còn ức chế cả chất vận chuyển monoamine trong túi synap gồm [[VMAT1]], [[VMAT2]], [[SLC1A1]], [[SLC22A3]] và [[SLC22A5]]. SLC1A1 là chất vận chuyển amino acid kích thích 3 (''Excitatory amino acid transporter 3'', EAAT3), một chất vận chuyển glutamat nằm trong tế bào thần kinh. SLC22A3 là chất vận chuyển monoamine ngoài thần kinh có trong [[Tế bào thần kinh đệm hình sao|tế bào thần kinh đệm hình hình sao]]. SLC22A5 là chất vận chuyển [[carnitine]] có ái lực cao. Amphetamin làm tăng [[biểu hiện gen]] [[phiên mã điều hòa cocain và amphetamin]] (''cocaine- and amphetamin-regulated transcript'', CART).<ref name="CART NAcc">{{Chú thích tập san học thuật |vauthors=Vicentic A, Jones DC |date=February 2007 |title=The CART (cocaine- and amphetamine-regulated transcript) system in appetite and drug addiction |journal=Journal of Pharmacology and Experimental Therapeutics |volume=320 |issue=2 |pages=499–506 |doi=10.1124/jpet.105.091512 |pmid=16840648 |quote=The physiological importance of CART was further substantiated in numerous human studies demonstrating a role of CART in both feeding and psychostimulant addiction. ... Colocalization studies also support a role for CART in the actions of psychostimulants. ... CART and DA receptor transcripts colocalize (Beaudry et al., 2004). Second, dopaminergic nerve terminals in the NAc synapse on CART-containing neurons (Koylu et al., 1999), hence providing the proximity required for neurotransmitter signaling. These studies suggest that DA plays a role in regulating CART gene expression possibly via the activation of CREB.}}</ref> CART là [[neuropeptide]] liên quan đến hành vi ăn uống, căng thẳng và hành vi khen thưởng, gây ra sự gia tăng quá trình phát triển và tồn tại của các tế bào thần kinh ''[[In vitro|trong ống nghiệm]]''.<ref name="Drugbank-amph" /><ref name="CART functions">{{Chú thích tập san học thuật |vauthors=Zhang M, Han L, Xu Y |date=June 2012 |title=Roles of cocaine- and amphetamine-regulated transcript in the central nervous system |journal=Clinical and Experimental Pharmacology and Physiology |volume=39 |issue=6 |pages=586–592 |doi=10.1111/j.1440-1681.2011.05642.x |pmid=22077697 |quote=Recently, it was demonstrated that CART, as a neurotrophic peptide, had a cerebroprotective against focal ischaemic stroke and inhibited the neurotoxicity of β-amyloid protein, which focused attention on the role of CART in the central nervous system (CNS) and neurological diseases. ... The literature indicates that there are many factors, such as regulation of the immunological system and protection against energy failure, that may be involved in the cerebroprotection afforded by CART}}</ref><ref name="CART">{{Chú thích tập san học thuật |vauthors=Rogge G, Jones D, Hubert GW, Lin Y, Kuhar MJ |date=October 2008 |title=CART peptides: regulators of body weight, reward and other functions |journal=Nature Reviews Neuroscience |volume=9 |issue=10 |pages=747–758 |doi=10.1038/nrn2493 |pmc=4418456 |pmid=18802445 |quote=Several studies on CART (cocaine- and amphetamine-regulated transcript)-peptide-induced cell signalling have demonstrated that CART peptides activate at least three signalling mechanisms. First, CART 55–102 inhibited voltage-gated L-type Ca2+ channels ...}}</ref> Thụ thể CART vẫn chưa được xác định, nhưng có bằng chứng đáng kể cho thấy CART chỉ liên kết với [[Thụ thể bắt cặp với G protein|thụ thể bắt cặp với protein G]] (GPCR) ở đây là protein G<sub>i</sub> và G<sub>o</sub>.<ref name="CART" /><ref name="pmid21855138">{{Chú thích tập san học thuật |vauthors=Lin Y, Hall RA, Kuhar MJ |date=October 2011 |title=CART peptide stimulation of G protein-mediated signaling in differentiated PC12 cells: identification of PACAP 6–38 as a CART receptor antagonist |journal=Neuropeptides |volume=45 |issue=5 |pages=351–358 |doi=10.1016/j.npep.2011.07.006 |pmc=3170513 |pmid=21855138}}</ref> Amphetamin cũng ức chế [[monoamine oxidase]] ở liều rất cao, dẫn đến chuyển hóa monoamine và amine trace ít hơn. Hậu quả, nồng độ monoamine synap tăng.<ref name="PubChem Header">{{Chú thích bách khoa toàn thư|title=Amphetamine|publisher=United States National Library of Medicine – National Center for Biotechnology Information|access-date=17 April 2015|date=11 April 2015}}</ref><ref name="BRENDA MAO Homo sapiens">{{Chú thích bách khoa toàn thư|title=Monoamine oxidase (Homo sapiens)|publisher=Technische Universität Braunschweig|url=http://www.brenda-enzymes.info/enzyme.php?ecno=1.4.3.4&Suchword=&organism%5B%5D=Homo+sapiens&show_tm=0|access-date=4 May 2014|date=1 January 2014}}</ref> Ở người, thụ thể hiện tại được biết duy nhất ở màng sau synap mà amphetamin gắn được là [[Thụ thể 5-HT1A|thụ thể {{Nowrap|5-HT1A}}]].<ref name="5HT1A secondary">{{Chú thích bách khoa toàn thư|title=Amphetamine|publisher=University of Alberta|url=http://www.t3db.ca/toxins/T3D2706|access-date=24 February 2015}}</ref><ref name="5HT1A Primary">{{Chú thích tập san học thuật |vauthors=Toll L, Berzetei-Gurske IP, Polgar WE, Brandt SR, Adapa ID, Rodriguez L, Schwartz RW, Haggart D, O'Brien A, White A, Kennedy JM, Craymer K, Farrington L, Auh JS |date=March 1998 |title=Standard binding and functional assays related to medications development division testing for potential cocaine and opiate narcotic treatment medications |journal=NIDA Research Monograph |volume=178 |pages=440–466 |pmid=9686407}}</ref> |
|||
Tác dụng ngắn hạn của amphetamin ở người là do tăng cường dẫn truyền thần kinh, dưới tác dụng của [[Dopamin|dopamine]],<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref> [[serotonin]],<ref name="Miller" /> [[Norepinephrine|noradrenalin]],<ref name="Miller" /> [[adrenalin]],<ref name="E Weihe">{{Chú thích tập san học thuật |vauthors=Eiden LE, Weihe E |date=January 2011 |title=VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse |journal=Annals of the New York Academy of Sciences |volume=1216 |issue=1 |pages=86–98 |bibcode=<!-- No --> |doi=10.1111/j.1749-6632.2010.05906.x |pmc=4183197 |pmid=21272013 |quote=VMAT2 is the CNS vesicular transporter for not only the biogenic amines DA, NE, EPI, 5-HT, and HIS, but likely also for the trace amines TYR, PEA, and thyronamine (THYR) ... [Trace aminergic] neurons in mammalian CNS would be identifiable as neurons expressing VMAT2 for storage, and the biosynthetic enzyme aromatic amino acid decarboxylase (AADC). ... AMPH release of DA from synapses requires both an action at VMAT2 to release DA to the cytoplasm and a concerted release of DA from the cytoplasm via "reverse transport" through DAT.}}</ref> [[Histamin|histamine]],<ref name="E Weihe" /> [[Bảng điểm quy định cocain và amphetamine|CART peptide]],<ref name="CART NAcc">{{Chú thích tập san học thuật |vauthors=Vicentic A, Jones DC |date=February 2007 |title=The CART (cocaine- and amphetamine-regulated transcript) system in appetite and drug addiction |journal=Journal of Pharmacology and Experimental Therapeutics |volume=320 |issue=2 |pages=499–506 |doi=10.1124/jpet.105.091512 |pmid=16840648 |quote=The physiological importance of CART was further substantiated in numerous human studies demonstrating a role of CART in both feeding and psychostimulant addiction. ... Colocalization studies also support a role for CART in the actions of psychostimulants. ... CART and DA receptor transcripts colocalize (Beaudry et al., 2004). Second, dopaminergic nerve terminals in the NAc synapse on CART-containing neurons (Koylu et al., 1999), hence providing the proximity required for neurotransmitter signaling. These studies suggest that DA plays a role in regulating CART gene expression possibly via the activation of CREB.}}</ref> [[opioid nội sinh]],<ref name="Amphetamine-induced endogenous opioid release review">{{Chú thích tập san học thuật |vauthors=Finnema SJ, Scheinin M, Shahid M, Lehto J, Borroni E, Bang-Andersen B, Sallinen J, Wong E, Farde L, Halldin C, Grimwood S |date=November 2015 |title=Application of cross-species PET imaging to assess neurotransmitter release in brain |journal=Psychopharmacology |volume=232 |issue=21–22 |pages=4129–4157 |doi=10.1007/s00213-015-3938-6 |pmc=4600473 |pmid=25921033 |quote=More recently, Colasanti and colleagues reported that a pharmacologically induced elevation in endogenous opioid release reduced [<sup>11</sup>C]carfentanil binding in several regions of the human brain, including the basal ganglia, frontal cortex, and thalamus (Colasanti et al. 2012). Oral administration of d-amphetamine, 0.5 mg/kg, 3 h before [<sup>11</sup>C]carfentanil injection, reduced BPND values by 2–10%. The results were confirmed in another group of subjects (Mick et al. 2014). However, Guterstam and colleagues observed no change in [<sup>11</sup>C]carfentanil binding when d-amphetamine, 0.3 mg/kg, was administered intravenously directly before injection of [<sup>11</sup>C]carfentanil (Guterstam et al. 2013). It has been hypothesized that this discrepancy may be related to delayed increases in extracellular opioid peptide concentrations following amphetamine-evoked monoamine release (Colasanti et al. 2012; Mick et al. 2014).}}</ref><ref name="Opioids">{{Chú thích tập san học thuật |vauthors=Loseth GE, Ellingsen DM, Leknes S |date=December 2014 |title=State-dependent μ-opioid modulation of social motivation |journal=Frontiers in Behavioral Neuroscience |volume=8 |pages=430 |doi=10.3389/fnbeh.2014.00430 |pmc=4264475 |pmid=25565999 |quote=Similar MOR activation patterns were reported during positive mood induced by an amusing video clip (Koepp et al., 2009) and following amphetamine administration in humans (Colasanti et al., 2012). |doi-access=free}}</ref><ref name="Opioids cited primary source">{{Chú thích tập san học thuật |vauthors=Colasanti A, Searle GE, Long CJ, Hill SP, Reiley RR, Quelch D, Erritzoe D, Tziortzi AC, Reed LJ, Lingford-Hughes AR, Waldman AD, Schruers KR, Matthews PM, Gunn RN, Nutt DJ, Rabiner EA |date=September 2012 |title=Endogenous opioid release in the human brain reward system induced by acute amphetamine administration |journal=Biological Psychiatry |volume=72 |issue=5 |pages=371–377 |doi=10.1016/j.biopsych.2012.01.027 |pmid=22386378}}</ref> [[hormone vỏ thượng thận]],<ref name="Human amph effects">{{Chú thích sách|title=Drug Addiction II: Amphetamine, Psychotogen, and Marihuana Dependence|last=Gunne LM|date=2013|publisher=Springer|isbn=9783642667091|location=Berlin, Germany; Heidelberg, Germany|pages=247–260|chapter=Effects of Amphetamines in Humans|access-date=4 December 2015|chapter-url=https://books.google.com/books?id=gb_uCAAAQBAJ&pg=PA247}}</ref><ref name="Primary: Human HPA axis">{{Chú thích tập san học thuật |vauthors=Oswald LM, Wong DF, McCaul M, Zhou Y, Kuwabara H, Choi L, Brasic J, Wand GS |date=April 2005 |title=Relationships among ventral striatal dopamine release, cortisol secretion, and subjective responses to amphetamine |journal=Neuropsychopharmacology |volume=30 |issue=4 |pages=821–832 |doi=10.1038/sj.npp.1300667 |pmid=15702139 |quote=Findings from several prior investigations have shown that plasma levels of glucocorticoids and ACTH are increased by acute administration of AMPH in both rodents and humans |doi-access=free}}</ref> [[corticosteroid]],<ref name="Human amph effects" /><ref name="Primary: Human HPA axis" /> và [[Acid glutamic|glutamate]], thông qua tương tác với {{Abbr|CART|cocaine- and amphetamine-regulated transcript}}, {{Nowrap|{{abbr|5-HT1A|serotonin receptor 1A}}}}, {{Abbr|EAAT3|excitatory amino acid transporter 3}}, {{Abbr|TAAR1|trace amine-associated receptor 1}}, {{Abbr|VMAT1|vesicular monoamine transporter 1}}, {{Abbr|VMAT2|vesicular monoamine transporter 2}} và các [[mục tiêu sinh học]] khác. Amphetamin cũng kích hoạt 7 enzym [[Anhydrase cacbonic|carbonic anhydrase]], một trong 7 enzym này có mặt trong não người. |
|||
Dextroamphetamin là một chất chủ vận mạnh của {{Abbr|TAAR1|trace amine-associated receptor 1}} hơn levoamphetamin.<ref name="TAAR1 stereoselective" /> Do đó, dextroamphetamin tạo ra kích thích lên hệ TKTW lớn hơn levoamphetamin, gần gấp 3 đến 4 lần, nhưng levoamphetamin có tác dụng lên hệ tim mạch và tác dụng ngoại vi mạnh hơn.<ref name="Westfall">{{Chú thích sách|title=Goodman & Gilman's Pharmacological Basis of Therapeutics|vauthors=Westfall DP, Westfall TC|publisher=McGraw-Hill|year=2010|isbn=9780071624428|veditors=Brunton LL, Chabner BA, Knollmann BC|edition=12th|location=New York, USA|chapter=Miscellaneous Sympathomimetic Agonists}}</ref><ref name="TAAR1 stereoselective">{{Chú thích tập san học thuật |vauthors=Lewin AH, Miller GM, Gilmour B |date=December 2011 |title=Trace amine-associated receptor 1 is a stereoselective binding site for compounds in the amphetamine class |journal=Bioorganic & Medicinal Chemistry |volume=19 |issue=23 |pages=7044–7048 |doi=10.1016/j.bmc.2011.10.007 |pmc=3236098 |pmid=22037049}}</ref> |
|||
==== Dopamine ==== |
|||
Ở một số vùng não nhất định, amphetamin làm tăng nồng độ dopamine trong [[Synap hóa học|khe synap]].<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref> Amphetamin có thể xâm nhập vào [[Synap hóa học|tế bào thần kinh trước synap]] thông qua ''chất vận chuyển dopamine'' (DAT) hoặc bằng cách khuếch tán trực tiếp qua màng tế bào thần kinh.<ref name="Miller" /> Amphetamin ức chế tái hấp thu cạnh tranh ở chất vận chuyển dopamine.<ref name="Miller" /> Khi đi vào tế bào thần kinh trước synap, amphetamin sẽ kích hoạt {{Abbr|TAAR1|trace amine-associated receptor 1}} thông qua tín hiệu [[protein kinase A]] (PKA) và [[protein kinase C]] (PKC), gây ra quá trình [[phosphoryl hóa]] DAT.<ref name="Miller" /> Quá trình phosphoryl hóa nhờ PKC và PKA này dẫn đến [[nhập bào]] DAT (ức chế tái hấp thu không cạnh tranh), nhưng riêng sự phosphoryl hóa nhờ PKC gây ra sự vận chuyển ngược dopamine (tức là dopamine chui ra ngoài tế bào).<ref name="Miller" /><ref name="TAAR1 Review">{{Chú thích tập san học thuật |vauthors=Maguire JJ, Parker WA, Foord SM, Bonner TI, Neubig RR, Davenport AP |date=March 2009 |title=International Union of Pharmacology. LXXII. Recommendations for trace amine receptor nomenclature |journal=Pharmacological Reviews |volume=61 |issue=1 |pages=1–8 |doi=10.1124/pr.109.001107 |pmc=2830119 |pmid=19325074}}</ref> Amphetamin làm tăng nồng độ calci nội bào. Tác dụng này có liên quan đến quá trình phosphoryl hóa DAT thông qua con đường ''Ca2+/calmodulin-dependent protein kinase (CAMK''), làm thất thoát dopamin ra ngoài.<ref name="TAAR1 IUPHAR">{{Chú thích web|url=http://www.iuphar-db.org/DATABASE/ObjectDisplayForward?objectId=364|tựa đề=TA<sub>1</sub> receptor|ngày=2 December 2014|website=IUPHAR database|nhà xuất bản=International Union of Basic and Clinical Pharmacology|ngày truy cập=8 December 2014|trích dẫn=<!-- Comments: Tyramine causes an increase in intracellular cAMP in HEK293 or COS-7 cells expressing the TA1 receptor in vitro [4,6,18]. In addition, coupling to a promiscuous Gαq has been observed, resulting in increased intracellular calcium concentration [24]. -->}}</ref><ref name="DAT regulation review">{{Chú thích tập san học thuật |vauthors=Vaughan RA, Foster JD |date=September 2013 |title=Mechanisms of dopamine transporter regulation in normal and disease states |journal=Trends in Pharmacological Sciences |volume=34 |issue=9 |pages=489–496 |doi=10.1016/j.tips.2013.07.005 |pmc=3831354 |pmid=23968642 |quote=AMPH and METH also stimulate DA efflux, which is thought to be a crucial element in their addictive properties [80], although the mechanisms do not appear to be identical for each drug [81]. These processes are PKCβ– and CaMK–dependent [72, 82], and PKCβ knock-out mice display decreased AMPH-induced efflux that correlates with reduced AMPH-induced locomotion [72].}}</ref> Thông qua việc kích hoạt trực tiếp các ''kênh kali điều chỉnh bên trong bắt cặp với protein G'' (''G protein-coupled inwardly-rectifying potassium channel, GIRK''), {{Abbr|TAAR1|trace amine associated receptor 1}} làm giảm [[Điện thế hoạt động|tốc độ kích hoạt]] tế bào thần kinh dopamine, ngăn ngừa trạng thái cường dopaminergic.<ref name="GIRK">{{Chú thích tập san học thuật |vauthors=Ledonne A, Berretta N, Davoli A, Rizzo GR, Bernardi G, Mercuri NB |date=July 2011 |title=Electrophysiological effects of trace amines on mesencephalic dopaminergic neurons |journal=Frontiers in Systems Neuroscience |volume=5 |pages=56 |doi=10.3389/fnsys.2011.00056 |pmc=3131148 |pmid=21772817 |quote=Three important new aspects of TAs action have recently emerged: (a) inhibition of firing due to increased release of dopamine; (b) reduction of D2 and GABAB receptor-mediated inhibitory responses (excitatory effects due to disinhibition); and (c) a direct TA1 receptor-mediated activation of GIRK channels which produce cell membrane hyperpolarization. |doi-access=free}}</ref><ref name="Genatlas TAAR1">{{Chú thích web|url=http://genatlas.medecine.univ-paris5.fr/fiche.php?symbol=TAAR1|tựa đề=TAAR1|ngày=28 January 2012|website=GenAtlas|nhà xuất bản=University of Paris|ngày truy cập=29 May 2014|trích dẫn={{•}} tonically activates inwardly rectifying K(+) channels, which reduces the basal firing frequency of dopamine (DA) neurons of the ventral tegmental area (VTA)}}</ref><ref name="TAAR1-Paradoxical">{{Chú thích tập san học thuật |vauthors=Revel FG, Moreau JL, Gainetdinov RR, Bradaia A, Sotnikova TD, Mory R, Durkin S, Zbinden KG, Norcross R, Meyer CA, Metzler V, Chaboz S, Ozmen L, Trube G, Pouzet B, Bettler B, Caron MG, Wettstein JG, Hoener MC |date=May 2011 |title=TAAR1 activation modulates monoaminergic neurotransmission, preventing hyperdopaminergic and hypoglutamatergic activity |journal=Proceedings of the National Academy of Sciences |volume=108 |issue=20 |pages=8485–8490 |bibcode=<!-- No --> |doi=10.1073/pnas.1103029108 |pmc=3101002 |pmid=21525407 |doi-access=free}}</ref> |
|||
Amphetamin cũng là chất nền cho chất vận chuyển monoamine dạng túi synap, {{Abbr|VMAT2|vesicular monoamine transporter 2}}.<ref name="E Weihe">{{Chú thích tập san học thuật |vauthors=Eiden LE, Weihe E |date=January 2011 |title=VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse |journal=Annals of the New York Academy of Sciences |volume=1216 |issue=1 |pages=86–98 |bibcode=<!-- No --> |doi=10.1111/j.1749-6632.2010.05906.x |pmc=4183197 |pmid=21272013 |quote=VMAT2 is the CNS vesicular transporter for not only the biogenic amines DA, NE, EPI, 5-HT, and HIS, but likely also for the trace amines TYR, PEA, and thyronamine (THYR) ... [Trace aminergic] neurons in mammalian CNS would be identifiable as neurons expressing VMAT2 for storage, and the biosynthetic enzyme aromatic amino acid decarboxylase (AADC). ... AMPH release of DA from synapses requires both an action at VMAT2 to release DA to the cytoplasm and a concerted release of DA from the cytoplasm via "reverse transport" through DAT.}}</ref><ref name="Amphetamine VMAT2 pH gradient">{{Chú thích tập san học thuật |vauthors=Sulzer D, Cragg SJ, Rice ME |date=August 2016 |title=Striatal dopamine neurotransmission: regulation of release and uptake |journal=Basal Ganglia |volume=6 |issue=3 |pages=123–148 |doi=10.1016/j.baga.2016.02.001 |pmc=4850498 |pmid=27141430 |quote=Despite the challenges in determining synaptic vesicle pH, the proton gradient across the vesicle membrane is of fundamental importance for its function. Exposure of isolated catecholamine vesicles to protonophores collapses the pH gradient and rapidly redistributes transmitter from inside to outside the vesicle. ... Amphetamine and its derivatives like methamphetamine are weak base compounds that are the only widely used class of drugs known to elicit transmitter release by a non-exocytic mechanism. As substrates for both DAT and VMAT, amphetamines can be taken up to the cytosol and then sequestered in vesicles, where they act to collapse the vesicular pH gradient.}}</ref> Sau khi hấp thu amphetamin tại VMAT2, amphetamin làm vỡ các túi synap ở khe synap, giải phóng các phân tử dopamine từ các túi synap vào tế bào nhờ dòng chảy dopamine qua VMAT2.<ref name="E Weihe" /><ref name="Amphetamine VMAT2 pH gradient" /> Sau đó, các phân tử dopamine trong tế bào được giải phóng từ tế bào thần kinh trước synap vào khe synap thông qua sự vận chuyển thông qua ''chất vận chuyển dopamine'' (DAT) theo chiều ngược lại.<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref><ref name="E Weihe" /><ref name="Amphetamine VMAT2 pH gradient" /> |
|||
==== Noradrenalin (norepinephrin) ==== |
|||
Tương tự như dopamine, liều amphetamin tùy thuộc vào mức độ của noradrenalin, tiền chất của [[adrenalin]].<ref name="cognition enhancers">{{Chú thích tập san học thuật |vauthors=Bidwell LC, McClernon FJ, Kollins SH |date=August 2011 |title=Cognitive enhancers for the treatment of ADHD |journal=Pharmacology Biochemistry and Behavior |volume=99 |issue=2 |pages=262–274 |doi=10.1016/j.pbb.2011.05.002 |pmc=3353150 |pmid=21596055}}</ref> Dựa trên biểu hiện {{Abbr|mRNA|messenger RNA}} của {{Abbr|TAAR1|trace amine-associated receptor 1}} trong neuron, amphetamin được cho là có tác động đến noradrenalin tương tự như dopamine.<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref><ref name="E Weihe">{{Chú thích tập san học thuật |vauthors=Eiden LE, Weihe E |date=January 2011 |title=VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse |journal=Annals of the New York Academy of Sciences |volume=1216 |issue=1 |pages=86–98 |bibcode=<!-- No --> |doi=10.1111/j.1749-6632.2010.05906.x |pmc=4183197 |pmid=21272013 |quote=VMAT2 is the CNS vesicular transporter for not only the biogenic amines DA, NE, EPI, 5-HT, and HIS, but likely also for the trace amines TYR, PEA, and thyronamine (THYR) ... [Trace aminergic] neurons in mammalian CNS would be identifiable as neurons expressing VMAT2 for storage, and the biosynthetic enzyme aromatic amino acid decarboxylase (AADC). ... AMPH release of DA from synapses requires both an action at VMAT2 to release DA to the cytoplasm and a concerted release of DA from the cytoplasm via "reverse transport" through DAT.}}</ref><ref name="TAAR1 Review">{{Chú thích tập san học thuật |vauthors=Maguire JJ, Parker WA, Foord SM, Bonner TI, Neubig RR, Davenport AP |date=March 2009 |title=International Union of Pharmacology. LXXII. Recommendations for trace amine receptor nomenclature |journal=Pharmacological Reviews |volume=61 |issue=1 |pages=1–8 |doi=10.1124/pr.109.001107 |pmc=2830119 |pmid=19325074}}</ref> Nói cách khác, amphetamin gây ra thất thoát noradrenalin nhờ TAAR1 và ức chế tái hấp thu ''không cạnh tranh'' tại chất vận chuyển noradrenalin được được phosphoryl hóa (''phosphorylated'' ''norepinephrine transporter'', ''phosphorylated'' ''NET''), ức chế tái hấp thu ''cạnh tranh'' tại chất vận chuyển noradrenalin (''norepinephrine transporter'', ''NET'') và giải phóng noradrenalin từ chất vận chuyển monoamine dạng túi synap {{Abbr|VMAT2|vesicular monoamine transporter 2}}.<ref name="Miller" /><ref name="E Weihe" /> |
|||
==== Serotonin ==== |
|||
Amphetamin có tác dụng tương tự trên serotonin như trên dopamine và norepinephrine (nhưng ít rõ rệt hơn).<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref><ref name="cognition enhancers">{{Chú thích tập san học thuật |vauthors=Bidwell LC, McClernon FJ, Kollins SH |date=August 2011 |title=Cognitive enhancers for the treatment of ADHD |journal=Pharmacology Biochemistry and Behavior |volume=99 |issue=2 |pages=262–274 |doi=10.1016/j.pbb.2011.05.002 |pmc=3353150 |pmid=21596055}}</ref> Amphetamin ảnh hưởng đến serotonin thông qua chất vận chuyển monoamine dạng túi synap {{Abbr|VMAT2|vesicular monoamine transporter 2}}. Giống cơ chế của noradrenalin, amphetamin làm thất thoát serotonin nhờ TAAR1 và ức chế tái hấp thu ''không cạnh tranh'' tại chất vận chuyển serotonin được được phosphoryl hóa (''phosphorylated'' ''serotonin transporter'', ''phosphorylated'' ''SERT'').<ref name="Miller" /><ref name="E Weihe">{{Chú thích tập san học thuật |vauthors=Eiden LE, Weihe E |date=January 2011 |title=VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse |journal=Annals of the New York Academy of Sciences |volume=1216 |issue=1 |pages=86–98 |bibcode=<!-- No --> |doi=10.1111/j.1749-6632.2010.05906.x |pmc=4183197 |pmid=21272013 |quote=VMAT2 is the CNS vesicular transporter for not only the biogenic amines DA, NE, EPI, 5-HT, and HIS, but likely also for the trace amines TYR, PEA, and thyronamine (THYR) ... [Trace aminergic] neurons in mammalian CNS would be identifiable as neurons expressing VMAT2 for storage, and the biosynthetic enzyme aromatic amino acid decarboxylase (AADC). ... AMPH release of DA from synapses requires both an action at VMAT2 to release DA to the cytoplasm and a concerted release of DA from the cytoplasm via "reverse transport" through DAT.}}</ref> Giống như dopamine, amphetamin có ái lực thấp với [[thụ thể 5-HT1A]] của người.<ref name="5HT1A secondary">{{Chú thích bách khoa toàn thư|title=Amphetamine|publisher=University of Alberta|url=http://www.t3db.ca/toxins/T3D2706|access-date=24 February 2015}}</ref><ref name="5HT1A Primary">{{Chú thích tập san học thuật |vauthors=Toll L, Berzetei-Gurske IP, Polgar WE, Brandt SR, Adapa ID, Rodriguez L, Schwartz RW, Haggart D, O'Brien A, White A, Kennedy JM, Craymer K, Farrington L, Auh JS |date=March 1998 |title=Standard binding and functional assays related to medications development division testing for potential cocaine and opiate narcotic treatment medications |journal=NIDA Research Monograph |volume=178 |pages=440–466 |pmid=9686407}}</ref> |
|||
==== Các chất dẫn truyền thần kinh, peptide, hormon và enzym khác ==== |
|||
Sử dụng amphetamin cấp tính ở người làm tăng giải phóng opioid nội sinh trong một số cấu trúc não thuộc [[hệ thống phần thưởng]].<ref name="Amphetamine-induced endogenous opioid release review">{{Chú thích tập san học thuật |vauthors=Finnema SJ, Scheinin M, Shahid M, Lehto J, Borroni E, Bang-Andersen B, Sallinen J, Wong E, Farde L, Halldin C, Grimwood S |date=November 2015 |title=Application of cross-species PET imaging to assess neurotransmitter release in brain |journal=Psychopharmacology |volume=232 |issue=21–22 |pages=4129–4157 |doi=10.1007/s00213-015-3938-6 |pmc=4600473 |pmid=25921033 |quote=More recently, Colasanti and colleagues reported that a pharmacologically induced elevation in endogenous opioid release reduced [<sup>11</sup>C]carfentanil binding in several regions of the human brain, including the basal ganglia, frontal cortex, and thalamus (Colasanti et al. 2012). Oral administration of d-amphetamine, 0.5 mg/kg, 3 h before [<sup>11</sup>C]carfentanil injection, reduced BPND values by 2–10%. The results were confirmed in another group of subjects (Mick et al. 2014). However, Guterstam and colleagues observed no change in [<sup>11</sup>C]carfentanil binding when d-amphetamine, 0.3 mg/kg, was administered intravenously directly before injection of [<sup>11</sup>C]carfentanil (Guterstam et al. 2013). It has been hypothesized that this discrepancy may be related to delayed increases in extracellular opioid peptide concentrations following amphetamine-evoked monoamine release (Colasanti et al. 2012; Mick et al. 2014).}}</ref><ref name="Opioids">{{Chú thích tập san học thuật |vauthors=Loseth GE, Ellingsen DM, Leknes S |date=December 2014 |title=State-dependent μ-opioid modulation of social motivation |journal=Frontiers in Behavioral Neuroscience |volume=8 |pages=430 |doi=10.3389/fnbeh.2014.00430 |pmc=4264475 |pmid=25565999 |quote=Similar MOR activation patterns were reported during positive mood induced by an amusing video clip (Koepp et al., 2009) and following amphetamine administration in humans (Colasanti et al., 2012). |doi-access=free}}</ref><ref name="Opioids cited primary source">{{Chú thích tập san học thuật |vauthors=Colasanti A, Searle GE, Long CJ, Hill SP, Reiley RR, Quelch D, Erritzoe D, Tziortzi AC, Reed LJ, Lingford-Hughes AR, Waldman AD, Schruers KR, Matthews PM, Gunn RN, Nutt DJ, Rabiner EA |date=September 2012 |title=Endogenous opioid release in the human brain reward system induced by acute amphetamine administration |journal=Biological Psychiatry |volume=72 |issue=5 |pages=371–377 |doi=10.1016/j.biopsych.2012.01.027 |pmid=22386378}}</ref> Khi tiếp xúc với amphetamin, nồng độ glutamat ngoại bào và nồng độ [[chất dẫn truyền thần kinh]] trong não được chứng minh là tăng trong thể vân. Sự gia tăng nồng độ glutamat ngoại bào này có lẽ xảy ra thông qua cơ chế liên quan đến [[EAAT3]] (một chất vận chuyển tái hấp thu glutamate) trong tế bào thần kinh dopamine. Amphetamin cũng gây ra sự giải phóng chọn lọc [[histamin]] từ [[Dưỡng bào|các tế bào mast]] và làm thoát histamin từ các tế bào thần kinh histaminergic thông qua {{Abbr|VMAT2|vesicular monoamine transporter 2}}.<ref name="E Weihe">{{Chú thích tập san học thuật |vauthors=Eiden LE, Weihe E |date=January 2011 |title=VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse |journal=Annals of the New York Academy of Sciences |volume=1216 |issue=1 |pages=86–98 |bibcode=<!-- No --> |doi=10.1111/j.1749-6632.2010.05906.x |pmc=4183197 |pmid=21272013 |quote=VMAT2 is the CNS vesicular transporter for not only the biogenic amines DA, NE, EPI, 5-HT, and HIS, but likely also for the trace amines TYR, PEA, and thyronamine (THYR) ... [Trace aminergic] neurons in mammalian CNS would be identifiable as neurons expressing VMAT2 for storage, and the biosynthetic enzyme aromatic amino acid decarboxylase (AADC). ... AMPH release of DA from synapses requires both an action at VMAT2 to release DA to the cytoplasm and a concerted release of DA from the cytoplasm via "reverse transport" through DAT.}}</ref> Sử dụng amphetamin làm tăng nồng độ hormone vỏ thượng thận và [[corticosteroid]] trong [[huyết tương]] bằng cách kích thích [[trục hạ đồi-tuyến yên-tuyến thượng thận]].<ref name="Evekeo">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f469fb38-0380-4621-9db3-a4f429126156|tựa đề=Evekeo- amphetamine sulfate tablet|ngày=14 August 2019|website=DailyMed|nhà xuất bản=Arbor Pharmaceuticals, LLC|ngày truy cập=22 December 2019}}</ref><ref name="Human amph effects">{{Chú thích sách|title=Drug Addiction II: Amphetamine, Psychotogen, and Marihuana Dependence|last=Gunne LM|date=2013|publisher=Springer|isbn=9783642667091|location=Berlin, Germany; Heidelberg, Germany|pages=247–260|chapter=Effects of Amphetamines in Humans|access-date=4 December 2015|chapter-url=https://books.google.com/books?id=gb_uCAAAQBAJ&pg=PA247}}</ref><ref name="Primary: Human HPA axis">{{Chú thích tập san học thuật |vauthors=Oswald LM, Wong DF, McCaul M, Zhou Y, Kuwabara H, Choi L, Brasic J, Wand GS |date=April 2005 |title=Relationships among ventral striatal dopamine release, cortisol secretion, and subjective responses to amphetamine |journal=Neuropsychopharmacology |volume=30 |issue=4 |pages=821–832 |doi=10.1038/sj.npp.1300667 |pmid=15702139 |quote=Findings from several prior investigations have shown that plasma levels of glucocorticoids and ACTH are increased by acute administration of AMPH in both rodents and humans |doi-access=free}}</ref> |
|||
Tháng 12 năm 2017, nghiên cứu đầu tiên đánh giá sự tương tác giữa amphetamin và enzym [[Anhydrase cacbonic|carbonic anhydrase]] ở người đã được công bố; trong số 11 enzym [[Anhydrase cacbonic|carbonic anhydrase]] được đưa vào nghiên cứu, amphetamin kích hoạt mạnh mẽ 7 enzym, trong đó có 4 enzym có mặt trong [[não người]]. Dựa trên nghiên cứu tiền lâm sàng, kích hoạt enzym [[Anhydrase cacbonic|carbonic anhydrase]] trong não có tác dụng nâng cao nhận thức.<ref name="Carbonic anhydrase modulators 2019 Review" /> Tuy nhiên, dựa trên việc sử dụng lâm sàng các [[chất ức chế carbonic anhydrase]], sự hoạt hóa [[Anhydrase cacbonic|carbonic anhydrase]] trong các mô khác có thể gây ra tác dụng phụ, chẳng hạn như làm trầm trọng thêm [[Cườm nước|bệnh glôcôm]].<ref name="Carbonic anhydrase modulators 2019 Review">{{Chú thích tập san học thuật |vauthors=Bozdag M, Altamimi AA, Vullo D, Supuran CT, Carta F |date=2019 |title=State of the Art on Carbonic Anhydrase Modulators for Biomedical Purposes |journal=Current Medicinal Chemistry |volume=26 |issue=15 |pages=2558–2573 |doi=10.2174/0929867325666180622120625 |pmid=29932025 |quote=CARBONIC ANHYDRASE INHIBITORS (CAIs). The design and development of CAIs represent the most prolific area within the CA research field. Since the introduction of CAIs in the clinical use in the 40', they still are the first choice for the treatment of edema [9], altitude sickness [9], glaucoma [7] and epilepsy [31]. ... CARBONIC ANHYDRASE ACTIVATORS (CAAs) ... The emerging class of CAAs has recently gained attraction as the enhancement of the kinetic properties in hCAs expressed in the CNS were proved in animal models to be beneficial for the treatment of both cognitive and memory impairments. Thus, CAAs have enormous potentiality in medicinal chemistry to be developed for the treatment of symptoms associated to aging, trauma or deterioration of the CNS tissues.}}</ref> |
|||
=== Dược động học === |
|||
[[Sinh khả dụng]] đường uống của amphetamine thay đổi theo pH đường tiêu hóa.<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref> Amphetamine được hấp thụ tốt ở ruột và sinh khả dụng thường trên 75% đối với dextroamphetamine. Amphetamine là một base yếu với [[Hằng số điện li acid|p''K''<sub>a</sub>]] là 9,9. Do đó, khi môi trường có pH kiềm, phần lớn hoạt chất nằm ở dạng [[base tự do]] hòa tan trong [[lipid]], và được hấp thu qua [[màng tế bào]] giàu lipid của [[biểu mô]] ruột.<ref name="FDA" /> Ngược lại, khi môi trường có pH toan, có nghĩa là hoạt chất chủ yếu ở dạng [[Ion|cation]] (muối) hòa tan trong nước và ít được hấp thu hơn. Khoảng {{Nowrap|20%}} amphetamine đi trong hệ tuần toàn được liên kết với [[Protein máu|protein huyết tương]]. Sau khi hấp thụ, amphetamine dễ dàng phân phối vào hầu hết các mô trong cơ thể. Amphetamine có nồng độ cao tại [[dịch não tủy]] và mô [[Não người|não]].<ref name="HSDB Toxnet October 2017 Full archived record">{{Chú thích bách khoa toàn thư|title=Amphetamine|publisher=Hazardous Substances Data Bank|url=http://toxnet.nlm.nih.gov/cgi-bin/sis/search/r?dbs+hsdb:@term+@rn+@rel+300-62-9|access-date=2 October 2017|archive-url=https://web.archive.org/web/20171002194327/https://toxnet.nlm.nih.gov/cgi-bin/sis/search2/cgi-bin/sis/search2/f?.%2Ftemp%2F~mdjW95%3A1%3AFULL|archive-date=2 October 2017|quote=Duration of effect varies depending on agent and urine pH. Excretion is enhanced in more acidic urine. Half-life is 7 to 34 hours and is, in part, dependent on urine pH (half-life is longer with alkaline urine). ... Amphetamines are distributed into most body tissues with high concentrations occurring in the brain and CSF. Amphetamine appears in the urine within about 3 hours following oral administration. ... Three days after a dose of (+ or -)-amphetamine, human subjects had excreted 91% of the (14)C in the urine}}</ref>The [[Biological half-life|half-lives]] of amphetamine enantiomers differ and vary with urine pH.<ref name="FDA Pharmacokinetics" /> At normal urine pH, the half-lives of dextroamphetamine and levoamphetamine are {{nowrap|9–11}} hours and {{nowrap|11–14}} hours, respectively.<ref name="FDA Pharmacokinetics" /> Highly acidic urine will reduce the enantiomer half-lives to 7 hours;<ref name="HSDB Toxnet October 2017 Full archived record" /> highly alkaline urine will increase the half-lives up to 34 hours.<ref name="HSDB Toxnet October 2017 Full archived record" /> The immediate-release and extended release variants of salts of both isomers reach [[Cmax (pharmacology)|peak plasma concentrations]] at 3 hours and 7 hours post-dose respectively.<ref name="FDA Pharmacokinetics" /> Amphetamine is [[Elimination (pharmacology)|eliminated]] via the [[kidney]]s, with {{nowrap|30–40%}} of the drug being excreted unchanged at normal urinary pH.<ref name="FDA Pharmacokinetics" /> When the urinary pH is basic, amphetamine is in its free base form, so less is excreted.<ref name="FDA Pharmacokinetics" /> When urine pH is abnormal, the urinary recovery of amphetamine may range from a low of 1% to a high of 75%, depending mostly upon whether urine is too basic or acidic, respectively.<ref name="FDA Pharmacokinetics" /> Following oral administration, amphetamine appears in urine within 3 hours.<ref name="HSDB Toxnet October 2017 Full archived record" /> Roughly 90% of ingested amphetamine is eliminated 3 days after the last oral dose.<ref name="HSDB Toxnet October 2017 Full archived record" />{{if pagename|Adderall=|Dextroamphetamine=|other= |
|||
Lisdexamfetamine is a [[prodrug]] of dextroamphetamine.<ref name="pmid27021968" /><ref name=USVyvanselabel /> It is not as sensitive to pH as amphetamine when being absorbed in the gastrointestinal tract.<ref name=USVyvanselabel>{{cite web | title=Vyvanse- lisdexamfetamine dimesylate capsule Vyvanse- lisdexamfetamine dimesylate tablet, chewable | website=DailyMed | publisher = Shire US Inc. | date=30 October 2019 | url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=704e4378-ca83-445c-8b45-3cfa51c1ecad | access-date=22 December 2019}}</ref> Following absorption into the blood stream, lisdexamfetamine is completely converted by [[red blood cell]]s to dextroamphetamine and the [[amino acid]] [[lysine|<small>L</small>-lysine]] by [[hydrolysis]] via undetermined [[aminopeptidase]] [[enzyme]]s.<ref name=USVyvanselabel/><ref name="pmid27021968" /><ref name="pmid28936175">{{cite journal | vauthors = Dolder PC, Strajhar P, Vizeli P, Hammann F, Odermatt A, Liechti ME | title = Pharmacokinetics and Pharmacodynamics of Lisdexamfetamine Compared with D-Amphetamine in Healthy Subjects | journal = Front Pharmacol | volume = 8 | issue = | pages = 617 | date = 2017 | pmid = 28936175 | pmc = 5594082 | doi = 10.3389/fphar.2017.00617 | url = | quote = Inactive lisdexamfetamine is completely (>98%) converted to its active metabolite D-amphetamine in the circulation (Pennick, 2010; Sharman and Pennick, 2014). When lisdexamfetamine is misused intranasally or intravenously, the pharmacokinetics are similar to oral use (Jasinski and Krishnan, 2009b; Ermer et al., 2011), and the subjective effects are not enhanced by parenteral administration in contrast to D-amphetamine (Lile et al., 2011) thus reducing the risk of parenteral misuse of lisdexamfetamine compared with D-amphetamine. Intravenous lisdexamfetamine use also produced significantly lower increases in "drug liking" and "stimulant effects" compared with D-amphetamine in intravenous substance users (Jasinski and Krishnan, 2009a).| doi-access = free }}</ref> This is the [[rate-limiting step]] in the [[bioactivation]] of lisdexamfetamine.<ref name="pmid27021968" /> The elimination half-life of lisdexamfetamine is generally less than 1 hour.<ref name=USVyvanselabel /><ref name="pmid27021968" /> Due to the necessary conversion of lisdexamfetamine into dextroamphetamine, levels of dextroamphetamine with lisdexamfetamine peak about one hour later than with an equivalent dose of immediate-release dextroamphetamine.<ref name="pmid27021968">{{cite journal | vauthors = Ermer JC, Pennick M, Frick G | title = Lisdexamfetamine Dimesylate: Prodrug Delivery, Amphetamine Exposure and Duration of Efficacy | journal = Clinical Drug Investigation | volume = 36 | issue = 5 | pages = 341–356 | date = May 2016 | pmid = 27021968 | pmc = 4823324 | doi = 10.1007/s40261-015-0354-y }}</ref><ref name="pmid28936175" /> Presumably due to its rate-limited activation by red blood cells, [[intravenous administration]] of lisdexamfetamine shows greatly delayed time to peak and reduced peak levels compared to intravenous administration of an equivalent dose of dextroamphetamine.<ref name="pmid27021968" /> The pharmacokinetics of lisdexamfetamine are similar regardless of whether it is administered orally, [[intranasal administration|intranasally]], or intravenously.<ref name="pmid27021968" /><ref name="pmid28936175" /> Hence, in contrast to dextroamphetamine, [[parenteral administration|parenteral]] use does not enhance the subjective effects of lisdexamfetamine.<ref name="pmid27021968" /><ref name="pmid28936175" /> Because of its behavior as a prodrug and its pharmacokinetic differences, lisdexamfetamine has a longer duration of therapeutic effect than immediate-release dextroamphetamine and shows reduced misuse potential.<ref name="pmid27021968" /><ref name="pmid28936175" />}} |
|||
Cho đến hiện tịa, [[CYP2D6]], [[dopamine β-hydroxylase]] (DBH), [[Monooxygenase 3 chứa flavin|monooxygenase chứa flavin 3]] (''flavin-containing monooxygenase 3'', FMO3), [[butyrate-CoA ligase]] (XM-ligase), và [[Glycine N-acyltransferase|glycine ''N''-acyltransferase]] (GLYAT) là các enzym được biết đến có tham gia chuyển hóa amphetamin hoặc các chất trung gian ở người. Amphetamin có nhiều loại sản phẩm chuyển hóa gồm {{Nowrap|[[4-hydroxyamphetamine]]}}, {{Nowrap|[[4-hydroxynorephedrine]]}}, {{Nowrap|[[4-hydroxyphenylacetone]]}}, [[acid benzoic]], [[acid hippuric]], [[Phenylpropanolamine|norephedrine]] và [[Phenylacetone|phenylaceton]]. Trong số các chất chuyển hóa này, chất [[Thuốc kích thích giao cảm|kích thích giao cảm]] có hoạt tính là {{Nowrap|4-hydroxyamphetamine}},<ref>{{Chú thích bách khoa toàn thư|title=p-Hydroxyamphetamine|publisher=United States National Library of Medicine – National Center for Biotechnology Information|access-date=15 October 2013}}</ref> {{Nowrap|4-hydroxynorephedrine}},<ref>{{Chú thích bách khoa toàn thư|title=p-Hydroxynorephedrine|publisher=United States National Library of Medicine – National Center for Biotechnology Information|access-date=15 October 2013}}</ref> và norephedrine.<ref>{{Chú thích bách khoa toàn thư|title=Phenylpropanolamine|publisher=United States National Library of Medicine – National Center for Biotechnology Information|access-date=15 October 2013}}</ref> Các con đường chuyển hóa chính liên quan đến quá trình para-hydroxyl hóa nhân thơm, alpha- và betahydroxyl hóa hợp chất không vòng, ''N-''oxy hóa'', N-''dealkyl hóa, và khử amin.<ref name="Pubchem Kinetics">{{Chú thích bách khoa toàn thư|title=Amphetamine|publisher=United States National Library of Medicine – National Center for Biotechnology Information|access-date=12 October 2013}}</ref> Các con đường trao đổi chất, các chất trung gian chuyển hóa đã được phát hiện và các enzym chuyển hóa ở người được trình bày trong sơ đồ dưới đây:{{Amphetamine pharmacokinetics|caption=The primary active metabolites of amphetamine are {{nowrap|4-hydroxyamphetamine}} and norephedrine;<ref name="Metabolites" /> at normal urine pH, about {{nowrap|30–40%}} of amphetamine is excreted unchanged and roughly 50% is excreted as the inactive metabolites (bottom row).<ref name="FDA Pharmacokinetics" /> The remaining {{nowrap|10–20%}} is excreted as the active metabolites.<ref name="FDA Pharmacokinetics" /> Benzoic acid is metabolized by {{abbr|XM-ligase|butyrate-CoA ligase}} into an intermediate product, [[benzoyl-CoA]], which is then metabolized by {{abbr|GLYAT|glycine ''N''-acyltransferase}} into hippuric acid.<ref name="Glycine conjugation review" />}}{{Amphetamine pharmacokinetics|caption=The primary active metabolites of amphetamine are {{nowrap|4-hydroxyamphetamine}} and norephedrine;<ref name="Metabolites" /> at normal urine pH, about {{nowrap|30–40%}} of amphetamine is excreted unchanged and roughly 50% is excreted as the inactive metabolites (bottom row).<ref name="FDA Pharmacokinetics" /> The remaining {{nowrap|10–20%}} is excreted as the active metabolites.<ref name="FDA Pharmacokinetics" /> Benzoic acid is metabolized by {{abbr|XM-ligase|butyrate-CoA ligase}} into an intermediate product, [[benzoyl-CoA]], which is then metabolized by {{abbr|GLYAT|glycine ''N''-acyltransferase}} into hippuric acid.<ref name="Glycine conjugation review" />}}{{Clear}} |
|||
=== Dược-vi sinh-di truyền học (Pharmacomicrobiomic) === |
|||
[[Metagenomics|Metagenome]] của người (tức là các vật liệu di truyền của một cá thể và các vật liệu di truyền của tất cả các vi sinh vật có mặt trên hoặc bên trong cơ thể của cá thể đó) rõ ràng là rất khác nhau giữa các cá thể.<ref name="Pharmacomicrobiomics">{{Chú thích tập san học thuật |vauthors=ElRakaiby M, Dutilh BE, Rizkallah MR, Boleij A, Cole JN, Aziz RK |date=July 2014 |title=Pharmacomicrobiomics: the impact of human microbiome variations on systems pharmacology and personalized therapeutics |journal=Omics |volume=18 |issue=7 |pages=402–414 |doi=10.1089/omi.2014.0018 |pmc=4086029 |pmid=24785449 |quote=The hundred trillion microbes and viruses residing in every human body, which outnumber human cells and contribute at least 100 times more genes than those encoded on the human genome (Ley et al., 2006), offer an immense accessory pool for inter-individual genetic variation that has been underestimated and largely unexplored (Savage, 1977; Medini et al., 2008; Minot et al., 2011; Wylie et al., 2012). ... Meanwhile, a wealth of literature has long been available about the biotransformation of xenobiotics, notably by gut bacteria (reviewed in Sousa et al., 2008; Rizkallah et al., 2010; Johnson et al., 2012; Haiser and Turnbaugh, 2013). This valuable information is predominantly about drug metabolism by unknown human-associated microbes; however, only a few cases of inter-individual microbiome variations have been documented [e.g., digoxin (Mathan et al., 1989) and acetaminophen (Clayton et al., 2009)].}}</ref><ref name="Human microbiome">{{Chú thích tập san học thuật |vauthors=Cho I, Blaser MJ |date=March 2012 |title=The human microbiome: at the interface of health and disease |journal=Nature Reviews Genetics |volume=13 |issue=4 |pages=260–270 |doi=10.1038/nrg3182 |pmc=3418802 |pmid=22411464 |quote=The composition of the microbiome varies by anatomical site (Figure 1). The primary determinant of community composition is anatomical location: interpersonal variation is substantial<sup>23,24</sup> and is higher than the temporal variability seen at most sites in a single individual<sup>25</sup>. ... How does the microbiome affect the pharmacology of medications? Can we "micro-type" people to improve pharmacokinetics and/or reduce toxicity? Can we manipulate the microbiome to improve pharmacokinetic stability?}}</ref> Vì tổng số tế bào vi sinh vật và virus trong cơ thể người (hơn 100 nghìn tỷ) nhiều hơn rất nhiều tế bào người (hàng chục nghìn tỷ),<ref name="Pharmacomicrobiomics" /><ref name="Gut feeling">{{Chú thích tập san học thuật |vauthors=Hutter T, Gimbert C, Bouchard F, Lapointe FJ |year=2015 |title=Being human is a gut feeling |journal=Microbiome |volume=3 |pages=9 |doi=10.1186/s40168-015-0076-7 |pmc=4359430 |pmid=25774294 |quote=Some metagenomic studies have suggested that less than 10% of the cells that comprise our bodies are Homo sapiens cells. The remaining 90% are bacterial cells. The description of this so-called human microbiome is of great interest and importance for several reasons. For one, it helps us redefine what a biological individual is. We suggest that a human individual is now best described as a super-individual in which a large number of different species (including Homo sapiens) coexist.}}</ref> nên có khả năng tương tác đáng kể giữa thuốc và hệ vi sinh vật của một cá thể. Những tương tác đó bao gồm:<ref name="Pharmacomicrobiomics" /><ref name="Human microbiome" /><ref name="Microbial amphetamine metabolism - E. coli">{{Chú thích tập san học thuật |vauthors=Kumar K, Dhoke GV, Sharma AK, Jaiswal SK, Sharma VK |date=January 2019 |title=Mechanistic elucidation of amphetamine metabolism by tyramine oxidase from human gut microbiota using molecular dynamics simulations |journal=Journal of Cellular Biochemistry |volume=120 |issue=7 |pages=11206–11215 |doi=10.1002/jcb.28396 |pmid=30701587 |quote=<!--Numerous microorganisms reside with the human host in a symbiotic relationship and play an important role in the host metabolic processes and health.<sup>1,2</sup> Several studies in the recent past have reported that there are compositional differences in the human microbiome due to factors such as geographical location, diet, age, and genetic variations.<sup>3</sup>--> Particularly in the case of the human gut, which harbors a large diversity of bacterial species, the differences in microbial composition can significantly alter the metabolic activity in the gut lumen.<sup>4</sup> The differential metabolic activity due to the differences in gut microbial species has been recently linked with various metabolic disorders and diseases.<sup>5–12</sup> In addition to the impact of gut microbial diversity or dysbiosis in various human diseases, there is an increasing amount of evidence which shows that the gut microbes can affect the bioavailability and efficacy of various orally administrated drug molecules through promiscuous enzymatic metabolism.<sup>13,14</sup> ... The present study on the atomistic details of amphetamine binding and binding affinity to the tyramine oxidase along with the comparison with two natural substrates of this enzyme namely tyramine and phenylalanine provides strong evidence for the promiscuity-based metabolism of amphetamine by the tyramine oxidase enzyme of E. coli. The obtained results will be crucial in designing a surrogate molecule for amphetamine that can help either in improving the efficacy and bioavailability of the amphetamine drug via competitive inhibition or in redesigning the drug for better pharmacological effects. This study will also have useful clinical implications in reducing the gut microbiota caused variation in the drug response among different populations.}}</ref> |
|||
# thuốc làm thay đổi thành phần của [[hệ vi sinh vật]] ở người, |
|||
# vi sinh vật tiết các enzym làm thay đổi [[dược động học]] của thuốc |
|||
# sự chuyển hóa thuốc của vi sinh vật ảnh hưởng đến hiệu quả lâm sàng và [[độc tính]] của thuốc. |
|||
Lĩnh vực nghiên cứu những tương tác này được gọi là Dược-vi sinh-di truyền học (Pharmacomicrobiomic).<ref name="Pharmacomicrobiomics" /> |
|||
Tương tự như hầu hết các [[phân tử sinh học]] và [[chất lạ sinh học]] (''xenobiotic'')<ref>Thuật ngữ lấy từ [https://www.slideshare.net/hatoc5/chuyen-hoa-xenobiotic<nowiki>]</nowiki></ref> [[Thuốc dùng đường uống|dùng đường uống]], amphetamin sẽ phải trải qua quá trình chuyển hóa mạnh mẽ bởi [[Hệ vi sinh đường ruột|hệ vi khuẩn chí đường ruột của con người]] trước khi hấp thụ vào [[Hệ tuần hoàn|máu]].<ref name="Microbial amphetamine metabolism - E. coli">{{Chú thích tập san học thuật |vauthors=Kumar K, Dhoke GV, Sharma AK, Jaiswal SK, Sharma VK |date=January 2019 |title=Mechanistic elucidation of amphetamine metabolism by tyramine oxidase from human gut microbiota using molecular dynamics simulations |journal=Journal of Cellular Biochemistry |volume=120 |issue=7 |pages=11206–11215 |doi=10.1002/jcb.28396 |pmid=30701587 |quote=<!--Numerous microorganisms reside with the human host in a symbiotic relationship and play an important role in the host metabolic processes and health.<sup>1,2</sup> Several studies in the recent past have reported that there are compositional differences in the human microbiome due to factors such as geographical location, diet, age, and genetic variations.<sup>3</sup>--> Particularly in the case of the human gut, which harbors a large diversity of bacterial species, the differences in microbial composition can significantly alter the metabolic activity in the gut lumen.<sup>4</sup> The differential metabolic activity due to the differences in gut microbial species has been recently linked with various metabolic disorders and diseases.<sup>5–12</sup> In addition to the impact of gut microbial diversity or dysbiosis in various human diseases, there is an increasing amount of evidence which shows that the gut microbes can affect the bioavailability and efficacy of various orally administrated drug molecules through promiscuous enzymatic metabolism.<sup>13,14</sup> ... The present study on the atomistic details of amphetamine binding and binding affinity to the tyramine oxidase along with the comparison with two natural substrates of this enzyme namely tyramine and phenylalanine provides strong evidence for the promiscuity-based metabolism of amphetamine by the tyramine oxidase enzyme of E. coli. The obtained results will be crucial in designing a surrogate molecule for amphetamine that can help either in improving the efficacy and bioavailability of the amphetamine drug via competitive inhibition or in redesigning the drug for better pharmacological effects. This study will also have useful clinical implications in reducing the gut microbiota caused variation in the drug response among different populations.}}</ref> Enzyme vi sinh vật chuyển hóa amphetamin đầu tiên là [[Amin oxydase chính|tyramine oxidase]] do một chủng [[Escherichia coli|''vi khuẩn E. coli'']] tiết ra đã được xác định vào năm 2019.<ref name="Microbial amphetamine metabolism - E. coli" /> Enzyme chuyển hóa amphetamin, [[tyramin]] và phenethylamine với ái lực liên kết gần giống nhau đối với cả ba hợp chất.<ref name="Microbial amphetamine metabolism - E. coli">{{Chú thích tập san học thuật |vauthors=Kumar K, Dhoke GV, Sharma AK, Jaiswal SK, Sharma VK |date=January 2019 |title=Mechanistic elucidation of amphetamine metabolism by tyramine oxidase from human gut microbiota using molecular dynamics simulations |journal=Journal of Cellular Biochemistry |volume=120 |issue=7 |pages=11206–11215 |doi=10.1002/jcb.28396 |pmid=30701587 |quote=<!--Numerous microorganisms reside with the human host in a symbiotic relationship and play an important role in the host metabolic processes and health.<sup>1,2</sup> Several studies in the recent past have reported that there are compositional differences in the human microbiome due to factors such as geographical location, diet, age, and genetic variations.<sup>3</sup>--> Particularly in the case of the human gut, which harbors a large diversity of bacterial species, the differences in microbial composition can significantly alter the metabolic activity in the gut lumen.<sup>4</sup> The differential metabolic activity due to the differences in gut microbial species has been recently linked with various metabolic disorders and diseases.<sup>5–12</sup> In addition to the impact of gut microbial diversity or dysbiosis in various human diseases, there is an increasing amount of evidence which shows that the gut microbes can affect the bioavailability and efficacy of various orally administrated drug molecules through promiscuous enzymatic metabolism.<sup>13,14</sup> ... The present study on the atomistic details of amphetamine binding and binding affinity to the tyramine oxidase along with the comparison with two natural substrates of this enzyme namely tyramine and phenylalanine provides strong evidence for the promiscuity-based metabolism of amphetamine by the tyramine oxidase enzyme of E. coli. The obtained results will be crucial in designing a surrogate molecule for amphetamine that can help either in improving the efficacy and bioavailability of the amphetamine drug via competitive inhibition or in redesigning the drug for better pharmacological effects. This study will also have useful clinical implications in reducing the gut microbiota caused variation in the drug response among different populations.}}<cite class="citation journal cs1" data-ve-ignore="true" id="CITEREFKumarDhokeSharmaJaiswal2019">Kumar K, Dhoke GV, Sharma AK, Jaiswal SK, Sharma VK (January 2019). "Mechanistic elucidation of amphetamine metabolism by tyramine oxidase from human gut microbiota using molecular dynamics simulations". ''Journal of Cellular Biochemistry''. '''120''' (7): 11206–11215. [[DOI|doi]]:[[doi:10.1002/jcb.28396|10.1002/jcb.28396]]. [[PubMed|PMID]] [//pubmed.ncbi.nlm.nih.gov/30701587 30701587]. [[Semantic Scholar|S2CID]] [https://api.semanticscholar.org/CorpusID:73413138 73413138].<q>Particularly in the case of the human gut, which harbors a large diversity of bacterial species, the differences in microbial composition can significantly alter the metabolic activity in the gut lumen.<sup>4</sup> The differential metabolic activity due to the differences in gut microbial species has been recently linked with various metabolic disorders and diseases.<sup>5–12</sup> In addition to the impact of gut microbial diversity or dysbiosis in various human diseases, there is an increasing amount of evidence which shows that the gut microbes can affect the bioavailability and efficacy of various orally administrated drug molecules through promiscuous enzymatic metabolism.<sup>13,14</sup> ... The present study on the atomistic details of amphetamine binding and binding affinity to the tyramine oxidase along with the comparison with two natural substrates of this enzyme namely tyramine and phenylalanine provides strong evidence for the promiscuity-based metabolism of amphetamine by the tyramine oxidase enzyme of E. coli. The obtained results will be crucial in designing a surrogate molecule for amphetamine that can help either in improving the efficacy and bioavailability of the amphetamine drug via competitive inhibition or in redesigning the drug for better pharmacological effects. This study will also have useful clinical implications in reducing the gut microbiota caused variation in the drug response among different populations.</q></cite></ref> |
|||
=== Các hợp chất nội sinh liên quan === |
|||
Amphetamin có cấu trúc và chức năng rất giống với các trace amin [[wiktionary:endogenous|nội sinh]], là các phân tử [[điều hòa thần kinh]] tự nhiên được tạo ra trong cơ thể và não người.<ref name="Miller">{{Chú thích tập san học thuật |last=Miller GM |date=January 2011 |title=The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity |journal=Journal of Neurochemistry |volume=116 |issue=2 |pages=164–176 |doi=10.1111/j.1471-4159.2010.07109.x |pmc=3005101 |pmid=21073468}}</ref><ref name="Human trace amines and hTAARs October 2016 review">{{Chú thích tập san học thuật |vauthors=Khan MZ, Nawaz W |date=October 2016 |title=The emerging roles of human trace amines and human trace amine-associated receptors (hTAARs) in central nervous system |journal=Biomedicine & Pharmacotherapy |volume=83 |pages=439–449 |doi=10.1016/j.biopha.2016.07.002 |pmid=27424325}}</ref> Trong nhóm này, các hợp chất có liên quan chặt chẽ nhất là [[phenethylamin]] (hợp chất gốc của amphetamin) và {{Nowrap|[[N-methylphenethylamine|''N''-methylphenethylamine]]}} (một [[đồng phân]] của amphetamin, tức là {{Nowrap|[[N-methylphenethylamine|''N''-methylphenethylamine]]}} và amphetamin có công thức phân tử giống hệt nhau).<ref name="Miller" /><ref name="Renaissance GPCR">{{Chú thích tập san học thuật |vauthors=Lindemann L, Hoener MC |date=May 2005 |title=A renaissance in trace amines inspired by a novel GPCR family |journal=Trends in Pharmacological Sciences |volume=26 |issue=5 |pages=274–281 |doi=10.1016/j.tips.2005.03.007 |pmid=15860375 |quote=<!-- In addition to the main metabolic pathway, TAs can also be converted by nonspecific ''N''-methyltransferase (NMT) [22] and phenylethanolamine ''N''-methyltransferase (PNMT) [23] to the corresponding secondary amines (e.g. synephrine [14], ''N''-methylphenylethylamine and ''N''-methyltyramine [15]), which display similar activities on TAAR1 (TA1) as their primary amine precursors. -->}}</ref> Ở người, phenethylamine được sản xuất trực tiếp từ {{Nowrap|[[L-phenylalanine]]}} nhờ enzyme [[aromatic L-amino acid decarboxylase]] (AADC), enzyme này cũng chuyển {{Nowrap|[[L-DOPA]]}} thành dopamine.<ref name="Renaissance GPCR" /> Đổi lại, {{Nowrap|''N''-methylphenethylamine}} được chuyển hóa từ phenethylamine nhờ enzyme [[Phenylethanolamine N-methyltransferase|phenylethanolamine ''N'' -methyltransferase]] (cùng một loại enzyme chuyển hóa noreadrenalin thành adrenalin).<ref name="Renaissance GPCR" /> Giống như amphetamin, cả phenethylamine và {{Nowrap|''N''-methylphenethylamine}} có chức năng điều hòa dẫn truyền thần kinh monoamine thông qua {{Abbr|TAAR1|trace amine-associated receptor 1}}.<ref name="Miller" /><ref name="Human trace amines and hTAARs October 2016 review" /><ref name="Renaissance GPCR" /> Tuy nhiên, không giống như amphetamin, cả hai chất này đều bị phân hủy bởi [[monoamine oxidase B]], và do đó có thời gian bán hủy ngắn hơn amphetamin.<ref name="Renaissance GPCR" /> |
|||
== Hoá học == |
|||
<!--Chemical data--> |
|||
{{Annotated image 4|caption=Công thức cấu tạo của {{nowrap|{{abbr|L-amph|levoamphetamin}}}} và {{nowrap|{{abbr|D-amph|dextroamphetamin}}}}|header=Hỗn hợp [[racemic]] của amphetamin|header_align=center|header_background=aliceblue|alt=Graphical representation of Amphetamine stereoisomers|image=Racemic_amphetamine.svg|align=right|image-width=300|image-left=0|image-top=0|width=300|height=76|annot-font-size=14|annot-text-align=left|annotations={{Annotation|5|60|[[Levoamphetamin]]}} |
|||
| C=9 | H=13 | N=1 |
|||
{{Annotation|170|60|[[Dextroamphetamin]]}}}}{{Nhiều hình |
|||
| molecular_weight = 135.2084 |
|||
| align = right |
|||
| smiles = NC(C)Cc1ccccc1 |
|||
| direction = vertical |
|||
| InChI = 1/C9H13N/c1-8(10)7-9-5-3-2-4-6-9/h2-6,8H,7,10H2,1H3 |
|||
| width = 300 |
|||
| synonyms = alpha-methylbenzeneethanamine, alpha-methylphenethylamine, beta-phenyl-isopropylamine |
|||
<!-- Extra parameters -->| image1 = Amphetamine Freebase.png |
|||
| Boiling_Point = 203°C |
|||
| caption1 = A vial of the colorless amphetamine free base |
|||
| solubility = {{nowrap|50–100 mg/mL (16C°)}} |
|||
| alt1 = An image of amphetamine free base |
|||
| image2 = Amphetamine and P2P.png |
|||
| caption2 = Amphetamine hydrochloride (left bowl)<br />{{nowrap|[[Phenyl-2-nitropropene]]}} (right cups) |
|||
| alt2 = An image of phenyl-2-nitropropene and amphetamine hydrochloride |
|||
}} |
}} |
||
Amphetamin là một chất [[Dãy đồng đẳng|thuộc dãy đồng đẳng]] của chất dẫn truyền thần kinh phenethylamine động vật có vú. Công thức hóa học là {{Chem2|C9H13N|auto=yes}}. Nguyên tử carbon gắn nhóm chức [[amin]] là [[trung tâm lập thể]] và amphetamin được cấu tạo từ hỗn hợp racemic của hai [[Enantiomer|chất đối quang]] (''enantiomer'') với tỷ lệ 1:1. Hỗn hợp racemic này có thể phân tách thành các đồng phân quang học là [[levoamphetamin]] và [[dextroamphetamin]].<ref name="Drugbank-amph" /> Ở nhiệt độ phòng, dạng base tự do của amphetamin là chất [[Chất lỏng|lỏng]], không màu và dễ bay hơi với mùi [[amin]] đặc trưng, vị chát.<ref name="Properties">{{Chú thích bách khoa toàn thư|title=Amphetamine|publisher=United States National Library of Medicine – National Center for Biotechnology Information|access-date=13 October 2013}}</ref> Amphetamin dạng muối ở thể rắn, gồm amphetamin adipat,<ref>{{Chú thích web|url=https://www.federalregister.gov/documents/2003/11/10/03-28193/determination-that-delcobese-amphetamine-adipate-amphetamine-sulfate-dextroamphetamine-adipate|tựa đề=Determination That Delcobese (Amphetamine Adipate, Amphetamine Sulfate, Dextroamphetamine Adipate, Dextroamphetamine Sulfate) Tablets and Capsules Were Not Withdrawn From Sale for Reasons of Safety or Effectiveness|ngày=2003-11-10|website=Federal Register|ngày truy cập=2020-01-03}}</ref> aspartat,<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref> hydrochloride,<ref>{{Chú thích bách khoa toàn thư|title=Amphetamine Hydrochloride|publisher=United States National Library of Medicine – National Center for Biotechnology Information|url=https://pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=92939|access-date=8 November 2013}}</ref> phosphat,<ref>{{Chú thích bách khoa toàn thư|title=Amphetamine Phosphate|publisher=United States National Library of Medicine – National Center for Biotechnology Information|url=https://pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=62885|access-date=8 November 2013}}</ref> saccharat,<ref name="FDA" /> sulfat,<ref name="FDA" /> và tannat.<ref>{{Chú thích tập san học thuật |last=Cavallito |first=John |date=23 August 1960 |title=Amphetamine Tannate. Patent Application No. 2,950,309. |url=https://patentimages.storage.googleapis.com/23/7a/08/1e7b613dc61b17/US2950309.pdf |url-status=live |journal=United States Patent Office |archive-url=https://ghostarchive.org/archive/20221009/https://patentimages.storage.googleapis.com/23/7a/08/1e7b613dc61b17/US2950309.pdf |archive-date=2022-10-09}}</ref> Dextroamphetamin sulfat là muối enantiopure (có sẵn ở một dạng lập thể cụ thể) phổ biến nhất. Amphetamin cũng là hợp chất gốc [[Amphetamine thay thế|của lớp]] [[amphetamine thay thế|amphetamin thay thế]], gồm một số [[dẫn xuất]] có tác dụng lên thần kinh.<ref name="Drugbank-amph" /> Trong hóa học hữu cơ, amphetamin là một [[phối tử chiral]] (''chiral ligand'') rất hữu ích trong [[tổng hợp chọn lọc lập thể]] chất {{Nowrap|[[1,1'-bi-2-naphthol]]}}.<ref name="Chiral Ligand">{{Chú thích tập san học thuật |vauthors=Brussee J, Jansen AC |date=May 1983 |title=A highly stereoselective synthesis of s(−)-[1,1'-binaphthalene]-2,2'-diol |journal=Tetrahedron Letters |volume=24 |issue=31 |pages=3261–3262 |doi=10.1016/S0040-4039(00)88151-4}}</ref> |
|||
'''Amphetamine''' (hay còn gọi là hồng phiến)<ref>{{Chú thích web|url=http://www.molisa.gov.vn:80/Pages/tintuc/chitiet.aspx?TinTucID=23352&page=368|tựa đề=Hãy coi Người nghiện ma túy là người bệnh|website=www.molisa.gov.vn|ngôn ngữ=en-US|ngày truy cập=2022-04-16}}</ref> là loại [[Ma túy|ma tuý]] kích thích thần kinh trung ương [[Nghiện|gây nghiện]] từng được dùng để điều trị ADHD, chứng ngủ rũ, và béo phì. [[:en:Tolerance|Dung nạp]] thuốc ở Amphetamine tăng rất nhanh<ref>{{Chú thích web|url=http://www.merck.com/mmhe/sec07/ch108/ch108g.html|tựa đề=Amphetamines: Drug Use and Abuse: Merck Manual Home Edition|ngày=2007-02-17|website=web.archive.org|ngày truy cập=2022-04-16|archive-date=2007-02-17|archive-url=https://web.archive.org/web/20070217053619/http://www.merck.com/mmhe/sec07/ch108/ch108g.html|url-status=bot: unknown}}</ref>, phải sử dụng liều sau nhiều hơn liều trước để đạt được cùng một tác dụng như liều cũ. Do đó có thể dẫn đến nhiều hệ luỵ sức khoẻ nguy hiểm như hội chứng serotonin<ref>{{Chú thích tạp chí|last=Volpi-Abadie|first=Jacqueline|last2=Kaye|first2=Adam M.|last3=Kaye|first3=Alan David|date=2013|title=Serotonin Syndrome|url=https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3865832/|journal=The Ochsner Journal|volume=13|issue=4|pages=533–540|issn=1524-5012|pmc=3865832|pmid=24358002}}</ref>, chảy máu trong não, tim ngừng đập... vì quá liều. |
|||
== |
=== Các dẫn xuất === |
||
Các dẫn xuất của amphetamin, hoặc "amphetamin thay thế", là các hợp chất sử dụng cấu trúc hóa học của amphetamin như một "xương sống".<ref name="Amphetamine - a substituted amphetamine">{{Chú thích tập san học thuật |vauthors=Hagel JM, Krizevski R, Marsolais F, Lewinsohn E, Facchini PJ |date=2012 |title=Biosynthesis of amphetamine analogs in plants |journal=Trends in Plant Science |volume=17 |issue=7 |pages=404–412 |doi=10.1016/j.tplants.2012.03.004 |pmid=22502775 |quote=Substituted amphetamines, which are also called phenylpropylamino alkaloids, are a diverse group of nitrogen-containing compounds that feature a phenethylamine backbone with a methyl group at the α-position relative to the nitrogen (Figure 1). ... Beyond (1''R'',2''S'')-ephedrine and (1''S'',2''S'')-pseudoephedrine, myriad other substituted amphetamines have important pharmaceutical applications. ... For example, (''S'')-amphetamine (Figure 4b), a key ingredient in Adderall and Dexedrine, is used to treat attention deficit hyperactivity disorder (ADHD) [79]. ...<br>[Figure 4](b) Examples of synthetic, pharmaceutically important substituted amphetamines.}}</ref><ref name="Schep">{{Chú thích tập san học thuật |vauthors=Schep LJ, Slaughter RJ, Beasley DM |date=August 2010 |title=The clinical toxicology of metamfetamine |journal=Clinical Toxicology |volume=48 |issue=7 |pages=675–694 |doi=10.3109/15563650.2010.516752 |issn=1556-3650 |pmid=20849327}}</ref> Nói một cách dễ hiểu, thay thế một hoặc nhiều nguyên tử hydro trong cấu trúc amphetamin bằng các [[nhóm thế]] sẽ tạo ra các dẫn xuất.<ref name="pmid1855720">{{Chú thích tập san học thuật |vauthors=Lillsunde P, Korte T |date=March 1991 |title=Determination of ring- and ''N''-substituted amphetamines as heptafluorobutyryl derivatives |journal=Forensic Science International |volume=49 |issue=2 |pages=205–213 |doi=10.1016/0379-0738(91)90081-s |pmid=1855720}}</ref> Các dẫn xuất amphetamin gồm các chất kích thần như [[methamphetamine|methamphetamin]], các chất kích thần và gây ảo giác qua cơ chế serotonergic như [[Thuốc lắc|MDMA]] (thuốc lắc) và [[thuốc thông mũi]] như [[ephedrin]], v.v....<ref name="Amphetamine - a substituted amphetamine" /><ref name="Schep" /> |
|||
Amphetamin được tổng hợp lần đầu tiên vào năm [[1887]]. Bốn mươi năm sau, đặc tính kích thích của loại thuốc này được khám phá. Sau đó, vào năm 1932, lần đầu tiên nó xuất hiện trên thị trường [[Hoa Kỳ]] dưới dạng thuốc hít. Amphetamin trở nên phổ biến vào năm 1937, dưới dạng viên, với tác dụng chữa chứng ngủ rũ.<ref name=erowidvault>{{chú thích web|author=Amphetamines |url=http://www.erowid.org/chemicals/amphetamines/amphetamines_effects.shtml |title=Erowid Amphetamines Vault | Effects |publisher=Erowid.org |date= |access-date =ngày 8 tháng 5 năm 2012}}</ref><ref name = "strdbo">{{Chú thích web |url=http://www.xs4all.nl/~4david/amphetam.html |ngày truy cập=2012-10-13 |tựa đề=Amphetamine; Facts {{!}} Alcoholism and Drug Addiction Research Foundation, Toronto Canada |archive-date = ngày 12 tháng 11 năm 1999 |archive-url=https://web.archive.org/web/19991112225253/http://www.xs4all.nl/~4david/amphetam.html |url-status=dead }}</ref><ref>{{chú thích web |url=http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Amphetamines |title=Amphetamines | Better Health Channel |publisher=Betterhealth.vic.gov.au |date=ngày 25 tháng 1 năm 2012 |access-date=ngày 8 tháng 5 năm 2012 |archive-date=2012-10-22 |archive-url=https://web.archive.org/web/20121022102531/http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Amphetamines |url-status=dead }}</ref><ref>{{chú thích web|url=http://www.mayoclinic.com/health/drug-information/DR602659#C5B63D57-E7FF-0DBD-1B31F9CC4EA63178 |title=Dextroamphetamine (Oral Route) |publisher=MayoClinic.com |date=ngày 1 tháng 11 năm 2011 |access-date =ngày 8 tháng 5 năm 2012}}</ref><ref>{{chú thích tạp chí |author=Vitiello B |title=Understanding the risk of using medications for attention deficit hyperactivity disorder with respect to physical growth and cardiovascular function |journal=Child Adolesc Psychiatr Clin N Am |volume=17 |issue=2 |pages=459–74, xi |year=2008|pmid=18295156 |pmc=2408826 |doi=10.1016/j.chc.2007.11.010}}</ref> Trong suốt [[Chiến tranh thế giới thứ hai|Thế chiến thứ 2]], amphetamin được sản xuất rất nhiều. Chất này vừa được sử dụng trong [[chiến tranh]] để tăng tỉnh táo, nhuệ khí cho binh lính.<ref name="Berman-2009">{{chú thích tạp chí | last1 = Berman | first1 = SM. | last2 = Kuczenski | first2 = R. | last3 = McCracken | first3 = JT. | last4 = London | first4 = ED. | title = Potential adverse effects of amphetamine treatment on brain and behavior: a review. | journal = Mol Psychiatry | volume = 14 | issue = 2 | pages = 123-42 | year = 2009 | doi = 10.1038/mp.2008.90 | PMID = 18698321 }}</ref><ref>{{chú thích web|url=http://www.merckmanuals.com/professional/special_subjects/drug_use_and_dependence/amphetamines.html |title=Amphetamines | Merck Sharp & Dohme Corp |publisher=Merckmanuals.com |date= |access-date =ngày 8 tháng 5 năm 2012}}</ref> |
|||
=== Tổng hợp === |
|||
Sau chiến tranh, có ba quốc gia xuất hiện những "dịch bệnh" sử dụng amphetamin. Dịch bệnh đầu tiên xuất hiện ở [[Nhật Bản]], bắt đầu từ năm 1945 và đỉnh điểm là năm 1954. Những công ty [[dược phẩm]] đã tung ra ngoài thị trường khi quân đội cắt hợp đồng, họ [[quảng cáo]] rộng rãi amphetamin cho cộng đồng. Nạn dịch này có tới 2 triệu người sử dụng amphetamin (thường bị [[quá liều]] khi dùng theo đường [[tĩnh mạch]]) với khoảng 550.000 người [[nghiện]], hầu hết ở độ tuổi từ 16 đến 25. Nạn dịch thứ hai xảy ra ở [[Thụy Điển|Thuỵ Điển]], cũng có đỉnh điểm vào giữa những năm 50 của thế kỷ 20, nhưng nó được xác nhận bởi phần những ca quá liều dùng theo đường tĩnh mạch tương tự [[phenmetrazin]]. |
|||
Năm 1887 ghi nhận quy trình đầu tiên tổng hợp amphetamin.<ref name="Vermont">{{Chú thích web|url=http://healthvermont.gov/adap/meth/brief_history.aspx|tựa đề=Historical overview of methamphetamine|website=Vermont Department of Health|nhà xuất bản=Government of Vermont|url lưu trữ=https://web.archive.org/web/20121005022228/http://healthvermont.gov/adap/meth/brief_history.aspx|ngày lưu trữ=5 October 2012|ngày truy cập=29 January 2012}}</ref> từ thời điểm đó trở đi, ngày càng có nhiều con đường tổng hợp amphetamin.<ref name="Allen_Ely_2009">{{Chú thích tập san học thuật |vauthors=Allen A, Ely R |date=April 2009 |title=Review: Synthetic Methods for Amphetamine |url=http://www.nwafs.org/newsletters/2011_Spring.pdf |journal=Crime Scene |publisher=Northwest Association of Forensic Scientists |volume=37 |issue=2 |pages=15–25 |access-date=6 December 2014}}</ref><ref name="Allen_Cantrell_1989">{{Chú thích tập san học thuật |vauthors=Allen A, Cantrell TS |date=August 1989 |title=Synthetic reductions in clandestine amphetamine and methamphetamine laboratories: A review |journal=Forensic Science International |volume=42 |issue=3 |pages=183–199 |doi=10.1016/0379-0738(89)90086-8}}</ref> Con đường phổ biến nhất của tổng hợp amphetamin hợp pháp và bất hợp pháp là sử dụng quá trình khử phi kim được gọi là [[phản ứng Leuckart]] ('''phương pháp 1''').<ref name="Amph Synth">{{Chú thích web|url=http://www.unodc.org/pdf/scientific/stnar34.pdf|tựa đề=Recommended methods of the identification and analysis of amphetamine, methamphetamine, and their ring-substituted analogues in seized materials|năm=2006|website=United Nations Office on Drugs and Crime|nhà xuất bản=United Nations|trang=9–12|ngày truy cập=14 October 2013}}</ref> Trong bước đầu tiên, phenylacetone phản ứng với [[formamide]], có thể bổ sung [[acid formic]], để tạo ra {{Nowrap|[[N-formylamphetamine|''N''-formylamphetamine]]}}. Chất trung gian này sau đó được thủy phân bằng cách sử dụng [[acid hydrochloric]], và sau đó base hóa, chiết xuất bằng dung môi hữu cơ, ngưng tụ và chưng cất để tạo ra dạng base tự do. Base tự do sau đó được hòa tan trong dung môi hữu cơ, thêm acid sulfuric, cho ra thành phẩm amphetamin kết tủa dưới dạng muối sulfat.<ref name="Amph Synth" /><ref>{{Chú thích tập san học thuật |vauthors=Pollard CB, Young DC |date=May 1951 |title=The Mechanism of the Leuckart Reaction |journal=The Journal of Organic Chemistry |volume=16 |issue=5 |pages=661–672 |doi=10.1021/jo01145a001}}</ref> |
|||
Một số phương pháp [[phân giải chiral]] (''chiral resolution'') được phát triển để tách hai đồng phân quang học của amphetamin.<ref name="Allen_Ely_2009">{{Chú thích tập san học thuật |vauthors=Allen A, Ely R |date=April 2009 |title=Review: Synthetic Methods for Amphetamine |url=http://www.nwafs.org/newsletters/2011_Spring.pdf |journal=Crime Scene |publisher=Northwest Association of Forensic Scientists |volume=37 |issue=2 |pages=15–25 |access-date=6 December 2014}}</ref> Ví dụ, hỗn hợp racemic amphetamin có thể được xử lý bằng {{Nowrap|d-[[tartaric acid]]}} để tạo thành một muối của [[đồng phân không đối quang]] (diastereomer), sau đó kết tinh [[Kết tinh phân đoạn (hóa học)|phân đoạn]] để tạo ra dextroamphetamin. Phân giải chiral vẫn là phương pháp kinh tế nhất để thu được amphetamin tinh khiết về mặt quang học trên quy mô lớn.<ref name="Gray_2007" /> Ngoài ra, một số quy trình tổng hợp chọn lọc lập thể của amphetamin đã được phát triển. Ví dụ, {{Nowrap|(''R'')-1-phenyl-ethanamine}} tinh khiết về mặt quang học được cô đặc với phenylacetone để tạo ra [[base Schiff]] chiral. Trong bước tổng hợp then chốt, chất trung gian này được khử bằng cách [[hydro hóa]], thay đổi tính đối xứng của nguyên tử carbon alpha bằng nhóm amin. Phân cắt liên kết amin [[Nhóm benzyl|benzylic]] bằng phản ứng hydro hóa tạo ra dextroamphetamin tinh khiết về mặt quang học.<ref name="Gray_2007">{{Chú thích sách|title=The Art of Drug Synthesis|last=Gray DL|publisher=Wiley-Interscience|year=2007|isbn=9780471752158|veditors=Johnson DS, Li JJ|location=New York, USA|page=247|chapter=Approved Treatments for Attention Deficit Hyperactivity Disorder: Amphetamine (Adderall), Methylphenidate (Ritalin), and Atomoxetine (Straterra)|chapter-url=https://books.google.com/books?id=zvruBDAulWEC&q=The%20Art%20of%20Drug%20Synthesis%20(Wiley%20Series%20on%20Drug%20Synthesis)&pg=SA17-PA4}}</ref> |
|||
==Tham khảo== |
|||
{{tham khảo|30em}} |
|||
==Liên kết ngoài== |
|||
* {{PubChemLink|5826}} ([[D-form]]—dextroamphetamine) |
|||
* {{PubChemLink|3007}} (L-form and D, L-forms) |
|||
* {{PubChemLink|32893}} ([[L-form]]—Levamphetamine or L-amphetamine) |
|||
* [http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pccompound&DbFrom=pccompound&Cmd=Link&LinkName=pccompound_pccompound&LinkReadableName=Similar%20Compounds&IdsFromResult=3007&ordinalpos=1&itool=EntrezSystem2.PEntrez.Pccompound.Pccompound_ResultsPanel.Pccompound_RVDocSum List of 504 Compounds Similar to Amphetamine (PubChem)] |
|||
* [http://www.emcdda.europa.eu/?nnodeid=25479 EMCDDA drugs profile: Amphetamine (2007)] |
|||
* [http://www.drugs.com/Amphetamine Drugs.com - Amphetamine] |
|||
* [http://www.apaic.org Asia & Pacific Amphetamine-Type Stimulants Information Centre] |
|||
* [http://druginfo.nlm.nih.gov/drugportal/dpdirect.jsp?name=Amphetamine U.S. National Library of Medicine: Drug Information Portal - Amphetamine] |
|||
Một số lượng lớn các con đường tổng hợp thay thế cho amphetamin đã được phát triển dựa trên các phản ứng hữu cơ cổ điển.<ref name="Allen_Ely_2009">{{Chú thích tập san học thuật |vauthors=Allen A, Ely R |date=April 2009 |title=Review: Synthetic Methods for Amphetamine |url=http://www.nwafs.org/newsletters/2011_Spring.pdf |journal=Crime Scene |publisher=Northwest Association of Forensic Scientists |volume=37 |issue=2 |pages=15–25 |access-date=6 December 2014}}</ref><ref name="Allen_Cantrell_1989">{{Chú thích tập san học thuật |vauthors=Allen A, Cantrell TS |date=August 1989 |title=Synthetic reductions in clandestine amphetamine and methamphetamine laboratories: A review |journal=Forensic Science International |volume=42 |issue=3 |pages=183–199 |doi=10.1016/0379-0738(89)90086-8}}</ref> |
|||
{{Sơ khai hóa học}} |
|||
{{thể loại Commons|Amphetamines}} |
|||
{{authority control}} |
|||
* [[Phản ứng Friedel-Crafts|Phản ứng Friedel – Crafts]] alkyl hóa [[benzen]] bằng [[allyl chloride]] để tạo ra beta chloropropylbenzen, sau đó phản ứng với amoniac để tạo ra racemic amphetamin ('''phương pháp 2''').<ref name="pmid20985610">{{Chú thích tập san học thuật |vauthors=Patrick TM, McBee ET, Hass HB |date=June 1946 |title=Synthesis of arylpropylamines; from allyl chloride |journal=Journal of the American Chemical Society |volume=68 |issue=6 |pages=1009–1011 |doi=10.1021/ja01210a032 |pmid=20985610}}</ref> |
|||
* [[Phản ứng Ritter]] ('''phương pháp 3'''). Trong con đường này, [[allylbenzen]] phản ứng với [[Acetonitrile|acetonitril]] trong acid sulfuric để tạo ra [[organosulfat]], sau đó cho phản ứng tiếp với natri hydroxide để tạo ra amphetamin thông qua chất trung gian [[acetamide]].<ref name="pmid18105933">{{Chú thích tập san học thuật |vauthors=Ritter JJ, Kalish J |date=December 1948 |title=A new reaction of nitriles; synthesis of t-carbinamines |journal=Journal of the American Chemical Society |volume=70 |issue=12 |pages=4048–4050 |doi=10.1021/ja01192a023 |pmid=18105933}}</ref><ref name="Krimen_Cota_1969">{{Chú thích sách|title=Organic Reactions|vauthors=Krimen LI, Cota DJ|date=March 2011|isbn=9780471264187|volume=17|page=216|chapter=The Ritter Reaction|doi=10.1002/0471264180.or017.03}}</ref> |
|||
* Alkyl hóa hợp chất {{Nowrap|[[ethyl acetoacetat|ethyl 3-oxobutanoat]]}} (còn gọi là ethyl acetoacetat) bằng [[Iodomethan|methyl iodide]], tiếp theo cho sản phẩm thu được phản ứng với [[benzyl chloride]] để chuyển thành acid {{Nowrap|2-methyl-3-phenyl-propanoic}}. Chất trung gian này chuyển vị thành amphetamin bằng cách sử dụng [[chuyển vị Hofmann]] hoặc [[chuyển vị Curtius]] ('''phương pháp 4'''). |
|||
Một số lượng đáng kể amphetamin được tổng hợp bằng cách [[Oxy hóa khử hữu cơ|khử]] nhóm [[Hợp chất nitro|nitro]], [[imine]], [[oxime]], hoặc các [[nhóm chức]] chứa nitơ khác.<ref name="Allen_Cantrell_1989">{{Chú thích tập san học thuật |vauthors=Allen A, Cantrell TS |date=August 1989 |title=Synthetic reductions in clandestine amphetamine and methamphetamine laboratories: A review |journal=Forensic Science International |volume=42 |issue=3 |pages=183–199 |doi=10.1016/0379-0738(89)90086-8}}</ref> |
|||
* [[Ngưng tụ Knoevenagel]] giữa [[benzaldehyde]] với [[nitroethan]] tạo ra {{Nowrap|[[phenyl-2-nitropropen]]}}. Liên kết đôi và nhóm nitro của chất trung gian này bị khử bằng cách [[hydro hóa]] có xúc tác hoặc khử bằng [[lithi nhôm hydride]] ([[Lithi|Li]][[Nhôm|Al]]H<sub>4</sub>) ('''phương pháp 5''').<ref name="Amph Synth">{{Chú thích web|url=http://www.unodc.org/pdf/scientific/stnar34.pdf|tựa đề=Recommended methods of the identification and analysis of amphetamine, methamphetamine, and their ring-substituted analogues in seized materials|năm=2006|website=United Nations Office on Drugs and Crime|nhà xuất bản=United Nations|trang=9–12|ngày truy cập=14 October 2013}}</ref><ref name="Delta Isotope">{{Chú thích tập san học thuật |vauthors=Collins M, Salouros H, Cawley AT, Robertson J, Heagney AC, Arenas-Queralt A |date=June 2010 |title=δ<sup>13</sup>C and δ<sup>2</sup>H isotope ratios in amphetamine synthesized from benzaldehyde and nitroethane |journal=Rapid Communications in Mass Spectrometry |volume=24 |issue=11 |pages=1653–1658 |bibcode=<!-- No --> |doi=10.1002/rcm.4563 |pmid=20486262}}</ref> |
|||
* Một phương pháp khác là phản ứng của [[Phenylacetone|phenylaceton]] với [[amonia]], tạo ra chất trung gian imine, sau đó sử dụng hydro có xúc tác paladi hoặc [[lithi nhôm hydride]] (LiAlH<sub>4</sub>) khử sản phẩm trên thành amin bậc một ('''phương pháp 6''').<ref name="Amph Synth" /> |
|||
=== Phát hiện trong dịch cơ thể === |
|||
Trong thể thao, công việc, hay để chẩn đoán [[ngộ độc]] và công tác giám định [[Khoa học pháp y|pháp y]] không thể thiếu các [[Xét nghiệm chất|xét nghiệm]] phát hiện amphetamin trong nước tiểu hoặc máu. [[Xét nghiệm miễn dịch]] là hình thức xét nghiệm amphetamin phổ biến nhất, tuy nhiên có thể [[phản ứng chéo]] với một số loại thuốc cường giao cảm.<ref name="NAHMSA_testing" /> Phương pháp sắc ký dành riêng cho amphetamin giúp hạn chế các kết quả dương tính giả.<ref name="pmid15516295" /> Kỹ thuật tách chiral giúp phân biệt nguồn gốc của thuốc, liệu là amphetamin kê đơn, amphetamin dạng tiền chất kê đơn, (ví dụ: [[Selegilin|selegiline]]), [[Thuốc không kê đơn|sản phẩm thuốc không kê đơn]] có chứa [[levomethamphetamine|levomethamphetamin]], [note 20] hay amphetamin thay thế do sản xuất bất hợp pháp.<ref name="pmid15516295">{{Chú thích tập san học thuật |vauthors=Paul BD, Jemionek J, Lesser D, Jacobs A, Searles DA |date=September 2004 |title=Enantiomeric separation and quantitation of (±)-amphetamine, (±)-methamphetamine, (±)-MDA, (±)-MDMA, and (±)-MDEA in urine specimens by GC-EI-MS after derivatization with (''R'')-(−)- or (''S'')-(+)-α-methoxy-α-(trifluoromethyl)phenylacetyl chloride (MTPA) |journal=Journal of Analytical Toxicology |volume=28 |issue=6 |pages=449–455 |doi=10.1093/jat/28.6.449 |pmid=15516295 |doi-access=free}}</ref><ref name="pmid16105261">{{Chú thích tập san học thuật |vauthors=Verstraete AG, Heyden FV |date=August 2005 |title=Comparison of the sensitivity and specificity of six immunoassays for the detection of amphetamines in urine |journal=Journal of Analytical Toxicology |volume=29 |issue=5 |pages=359–364 |doi=10.1093/jat/29.5.359 |pmid=16105261 |doi-access=free}}</ref><ref name="Baselt_2011">{{Chú thích sách|title=Disposition of Toxic Drugs and Chemicals in Man|last=Baselt RC|publisher=Biomedical Publications|year=2011|isbn=9780962652387|edition=9th|location=Seal Beach, USA|pages=85–88}}</ref> Một số loại thuốc kê đơn sản xuất amphetamin dưới dạng [[chất chuyển hóa]], bao gồm [[benzphetamine|benzphetamin]], [[clobenzorex]], [[famprofazone]], [[fenproporex]], [[lisdexamfetamine|lisdexamfetamin]], [[mesocarb]], methamphetamin, [[prenylamine]] và [[Selegilin|selegiline]],v...v.<ref name="Amph Uses">{{Chú thích tập san học thuật |vauthors=Heal DJ, Smith SL, Gosden J, Nutt DJ |date=June 2013 |title=Amphetamine, past and present – a pharmacological and clinical perspective |journal=Journal of Psychopharmacology |volume=27 |issue=6 |pages=479–496 |doi=10.1177/0269881113482532 |pmc=3666194 |pmid=23539642 |quote=The intravenous use of d-amphetamine and other stimulants still pose major safety risks to the individuals indulging in this practice. Some of this intravenous abuse is derived from the diversion of ampoules of d-amphetamine, which are still occasionally prescribed in the UK for the control of severe narcolepsy and other disorders of excessive sedation. ... For these reasons, observations of dependence and abuse of prescription d-amphetamine are rare in clinical practice, and this stimulant can even be prescribed to people with a history of drug abuse provided certain controls, such as daily pick-ups of prescriptions, are put in place (Jasinski and Krishnan, 2009b).}}</ref><ref name="pmid10711406">{{Chú thích tập san học thuật |last=Musshoff F |date=February 2000 |title=Illegal or legitimate use? Precursor compounds to amphetamine and methamphetamine |journal=Drug Metabolism Reviews |volume=32 |issue=1 |pages=15–44 |doi=10.1081/DMR-100100562 |pmid=10711406}}</ref><ref name="pmid12024689">{{Chú thích tập san học thuật |last=Cody JT |date=May 2002 |title=Precursor medications as a source of methamphetamine and/or amphetamine positive drug testing results |journal=Journal of Occupational and Environmental Medicine |volume=44 |issue=5 |pages=435–450 |doi=10.1097/00043764-200205000-00012 |pmid=12024689}}</ref> Xét nghiệm ma túy đối với những người sử dụng những dược chất trên có thể cho kết quả dương tính với amphetamin.<ref name="pmid10711406" /><ref name="pmid12024689" /> Amphetamin thường chỉ phát hiện được bằng xét nghiệm ma túy trong khoảng 24 giờ, mặc dù nếu dùng liều cao thì vẫn có thể phát hiện trong {{Nowrap|2–4}} ngày kể từ liều cuối cùng.<ref name="NAHMSA_testing">{{Chú thích web|url=http://www.ucdenver.edu/academics/colleges/PublicHealth/research/centers/CHWE/Documents/SAMHSA_drugtesting.pdf|tựa đề=Clinical Drug Testing in Primary Care|năm=2012|website=University of Colorado Denver|series=Technical Assistance Publication Series 32|nhà xuất bản=United States Department of Health and Human Services – Substance Abuse and Mental Health Services Administration|trang=55|url lưu trữ=https://web.archive.org/web/20180514022358/http://www.ucdenver.edu/academics/colleges/PublicHealth/research/centers/CHWE/Documents/SAMHSA_drugtesting.pdf|ngày lưu trữ=14 May 2018|url-status=live|ngày truy cập=31 October 2013|trích dẫn=A single dose of amphetamine or methamphetamine can be detected in the urine for approximately 24 hours, depending upon urine pH and individual metabolic differences. People who use chronically and at high doses may continue to have positive urine specimens for 2–4 days after last use (SAMHSA, 2010b).}}</ref> |
|||
Đối với các xét nghiệm, có nghiên cứu lưu ý rằng [[kỹ thuật xét nghiệm miễn dịch nhân lên bằng enzym]] (''Enzyme multiplied immunoassay technique'', EMIT) đối với amphetamin và methamphetamin có nhiều kết quả dương tính giả hơn so với phương pháp [[sắc ký lỏng-khối phổ]] (LC-MS).<ref name="pmid16105261">{{Chú thích tập san học thuật |vauthors=Verstraete AG, Heyden FV |date=August 2005 |title=Comparison of the sensitivity and specificity of six immunoassays for the detection of amphetamines in urine |journal=Journal of Analytical Toxicology |volume=29 |issue=5 |pages=359–364 |doi=10.1093/jat/29.5.359 |pmid=16105261 |doi-access=free}}</ref> [[Sắc ký khí-khối phổ]] (GC–MS)amphetamin và methamphetamin với thuốc thử dẫn xuất {{Nowrap|(''S'')-(−)-trifluoroacetylprolyl}} chloride cho phép phát hiện methamphetamin trong nước tiểu.<ref name="pmid15516295">{{Chú thích tập san học thuật |vauthors=Paul BD, Jemionek J, Lesser D, Jacobs A, Searles DA |date=September 2004 |title=Enantiomeric separation and quantitation of (±)-amphetamine, (±)-methamphetamine, (±)-MDA, (±)-MDMA, and (±)-MDEA in urine specimens by GC-EI-MS after derivatization with (''R'')-(−)- or (''S'')-(+)-α-methoxy-α-(trifluoromethyl)phenylacetyl chloride (MTPA) |journal=Journal of Analytical Toxicology |volume=28 |issue=6 |pages=449–455 |doi=10.1093/jat/28.6.449 |pmid=15516295 |doi-access=free}}</ref> GC–MS amphetamin và methamphetamin với thuốc thử chiral là [[acid Mosher]] cho phép phát hiện cả dextroamphetamin và dextromethamphetamin trong nước tiểu.<ref name="pmid15516295" /> Do đó, phương pháp này được sử dụng trên các mẫu có kết quả dương tính, giúp phân biệt nguồn gốc của thuốc.<ref name="pmid15516295" /> |
|||
== Lịch sử, xã hội và văn hóa == |
|||
{{Global estimates of illegal drug users}}Chất kích thích dạng amphetamin ban đầu có nguồn gốc từ cây ''[[Chi Ma hoàng|Ma hoàng]]'', có chứa [[ephedrin]], được người [[Trung Quốc]] sử dụng khoảng 5.000 trước.<ref name="pmid34000249">{{Chú thích tập san học thuật |vauthors=Morelli M, Tognotti E |date=August 2021 |title=Brief history of the medical and non-medical use of amphetamine-like psychostimulants |url= |journal=Exp Neurol |volume=342 |issue= |pages=113754 |doi=10.1016/j.expneurol.2021.113754 |pmid=34000249}}</ref><ref name="pmid24344115">{{Chú thích tập san học thuật |vauthors=Wood S, Sage JR, Shuman T, Anagnostaras SG |date=2014 |title=Psychostimulants and cognition: a continuum of behavioral and cognitive activation |url= |journal=Pharmacol Rev |volume=66 |issue=1 |pages=193–221 |doi=10.1124/pr.112.007054 |pmc=3880463 |pmid=24344115}}</ref> Ephedrin được phân lập từ ''[[Ephedra distachya|Ephedra vulgaris]]'' ở [[Nhật Bản]] vào năm 1885 và được nghiên cứu các đặc tính y học của cây trong suốt thập niên 1920.<ref name="pmid34000249" /> Do hàm lượng ephedrin trong cây ''Ephedra'' quá ít nên đã thúc đẩy việc tìm kiếm chất tương tựephedrin.<ref name="pmid34000249" /> |
|||
Amphetamin được tổng hợp lần đầu tiên vào năm 1887 tại Đức, do nhà hóa học người Romania [[Lazăr Edeleanu]]. Ông đặt tên cho chất là ''phenylisopropylamine'';<ref name="Vermont">{{Chú thích web|url=http://healthvermont.gov/adap/meth/brief_history.aspx|tựa đề=Historical overview of methamphetamine|website=Vermont Department of Health|nhà xuất bản=Government of Vermont|url lưu trữ=https://web.archive.org/web/20121005022228/http://healthvermont.gov/adap/meth/brief_history.aspx|ngày lưu trữ=5 October 2012|ngày truy cập=29 January 2012}}</ref><ref>{{Chú thích sách|title=Alcohol and Drug Misuse: A Handbook for Students and Health Professionals|last=Rassool GH|publisher=Routledge|year=2009|isbn=9780203871171|location=London, England|page=113}}</ref><ref name="SynthHistory" /> 40 năm sau, vào năm 1927, đặc tính kích thích của loại thuốc này được khám phá. Gordon Alles tái tổng hợp chất và cho rằng chất này có đặc tính [[Thuốc kích thích giao cảm|kích thích giao cảm]].<ref name="SynthHistory">{{Chú thích tập san học thuật |vauthors=Sulzer D, Sonders MS, Poulsen NW, Galli A |date=April 2005 |title=Mechanisms of neurotransmitter release by amphetamines: a review |journal=Progress in Neurobiology |volume=75 |issue=6 |pages=406–433 |doi=10.1016/j.pneurobio.2005.04.003 |pmid=15955613}}</ref> Cuối năm 1933, [[Smith, Kline và tiếng Pháp|Smith, Kline và French]] bắt đầu bán dưới dạng [[thuốc hít]], tên thương mại là Benzedrine, để làm thuốc thông mũi.<ref name="Benzedrine">{{Chú thích tập san học thuật |last=Rasmussen N |date=July 2006 |title=Making the first anti-depressant: amphetamine in American medicine, 1929–1950 |journal=Journal of the History of Medicine and Allied Sciences |volume=61 |issue=3 |pages=288–323 |doi=10.1093/jhmas/jrj039 |pmid=16492800 |quote=However the firm happened to discover the drug, SKF first packaged it as an inhaler so as to exploit the base's volatility and, after sponsoring some trials by East Coast otolaryngological specialists, began to advertise the Benzedrine Inhaler as a decongestant in late 1933.}}</ref> 3 năm sau, benzedrine sulfat được đưa vào sử dụng để điều trị nhiều loại [[bệnh]] lý khác nhau, bao gồm [[chứng ngủ rũ]], [[béo phì]], [[huyết áp thấp]], [[Thiếu hoặc mất ham muốn tình dục|giảm ham muốn]] ([[ICD-10]]: [[ICD-10 Chương 5: Rối loạn tâm thần và hành vi|F52.0]]) và [[Đau mãn tính|đau mạn tính]], v.v...<ref name="Benzedrine sulfate">{{Chú thích tập san học thuật |vauthors=Bett WR |date=August 1946 |title=Benzedrine sulphate in clinical medicine; a survey of the literature |journal=Postgraduate Medical Journal |volume=22 |issue=250 |pages=205–218 |doi=10.1136/pgmj.22.250.205 |pmc=2478360 |pmid=20997404}}</ref><ref name="Benzedrine" /> Trong Chiến tranh thế giới thứ hai, amphetamin và methamphetamin được sử dụng rộng rãi bởi cả [[Khối Đồng Minh thời Chiến tranh thế giới thứ hai|phe Đồng minh]] và [[phe Trục]] vì tác dụng kích thích và nâng cao độ tỉnh táo, nhuệ khí cho binh lính.<ref name="Vermont" /><ref>{{Chú thích tập san học thuật |last=Rasmussen N |date=August 2011 |title=Medical science and the military: the Allies' use of amphetamine during World War II |journal=Journal of Interdisciplinary History |volume=42 |issue=2 |pages=205–233 |doi=10.1162/JINH_a_00212 |pmid=22073434}}</ref><ref name="pmid22849208">{{Chú thích tập san học thuật |vauthors=Defalque RJ, Wright AJ |date=April 2011 |title=Methamphetamine for Hitler's Germany: 1937 to 1945 |journal=Bulletin of Anesthesia History |volume=29 |issue=2 |pages=21–24, 32 |doi=10.1016/s1522-8649(11)50016-2 |pmid=22849208}}</ref> Chính phủ các nước bắt đầu kiểm soát chặt chẽ việc bán amphetamin khi phát hiện các đặc tính gây nghiện của ma túy.<ref name="Vermont" /> Đầu những năm 1970 ở Hoa Kỳ, amphetamin được xếp vào danh sách chất phải kiểm soát theo Đạo luật Kiểm soát Chất.<ref>{{Chú thích web|url=https://www.fda.gov/regulatoryinformation/legislation/ucm148726.htm|tựa đề=Controlled Substances Act|ngày=11 June 2009|nhà xuất bản=United States Food and Drug Administration|url lưu trữ=https://web.archive.org/web/20170302014716/https://www.fda.gov/regulatoryinformation/legislation/ucm148726.htm|ngày lưu trữ=2 March 2017|ngày truy cập=4 November 2013}}</ref><ref>{{Chú thích web|url=https://www.deadiversion.usdoj.gov/schedules/|tựa đề=Controlled Substance Schedules|website=DEA Diversion Control Division|ngày truy cập=25 December 2019}}</ref> Bất chấp sự kiểm soát nghiêm ngặt của chính phủ, amphetamin vẫn được nhiều người thuộc đa ngành nghề, đa lĩnh vựng sử dụng hợp pháp hoặc bất hợp pháp, bao gồm các nhà văn,<ref>{{Chú thích web|url=http://www.wordsareimportant.com/ontheroad.htm|tựa đề=Forty Years of ''On the Road'' 1957–1997|tác giả=Gyenis A|website=wordsareimportant.com|nhà xuất bản=DHARMA beat|url lưu trữ=https://web.archive.org/web/20080214171739/http://www.wordsareimportant.com/ontheroad.htm|ngày lưu trữ=14 February 2008|ngày truy cập=18 March 2008}}</ref> nhạc sĩ,<ref>{{Chú thích tập san học thuật |last=Wilson A |year=2008 |title=Mixing the Medicine: The unintended consequence of amphetamine control on the Northern Soul Scene |url=http://www.internetjournalofcriminology.com/Wilson%20-%20Mixing%20the%20Medicine.pdf |journal=Internet Journal of Criminology |archive-url=https://web.archive.org/web/20110713045851/http://www.internetjournalofcriminology.com/Wilson%20-%20Mixing%20the%20Medicine.pdf |archive-date=13 July 2011 |access-date=25 May 2013}}</ref> nhà toán học,<ref>{{Chú thích web|url=http://www.untruth.org/~josh/math/Paul%20Erd%F6s%20bio-rev2.pdf|tựa đề=Paul Erdos, Mathematical Genius, Human (In That Order)|tác giả=Hill J|ngày=4 June 2004|ngày truy cập=2 November 2013}}</ref> và vận động viên. |
|||
Amphetamin ngày nay vẫn được tổng hợp bất hợp pháp trong các [[phòng thí nghiệm bí mật]] và được bán trên [[Kinh tế ngầm|thị trường chợ đen]], chủ yếu ở các nước châu Âu.<ref name="WDR2014">{{Chú thích web|url=https://www.unodc.org/documents/wdr2014/World_Drug_Report_2014_web.pdf|tựa đề=World Drug Report 2014|ngày=June 2014|editor=Mohan J|website=United Nations Office on Drugs and Crime|trang=3|ngày truy cập=18 August 2014}}</ref> {{Tính đến|2018}}, trong các quốc gia thành viên của Liên minh Châu Âu (EU), có 11,9 triệu người trưởng thành trong độ tuổi {{Nowrap|15–64}} đã sử dụng amphetamin hoặc methamphetamin ít nhất một lần trong đời và 1,7 hàng triệu người đã sử dụng trong năm 2017.<ref name="Bulletin2018">{{Chú thích web|url=http://www.emcdda.europa.eu/data/stats2018/gps_en|tựa đề=Statistical Bulletin 2018 − prevalence of drug use|nhà xuất bản=European Monitoring Centre for Drugs and Drug Addiction|ngày truy cập=5 February 2019}}</ref> Trong năm 2012, khoảng 5,9 [[tấn]] amphetamin bất hợp pháp đã bị thu giữ trong các nước thành viên EU.<ref name="EMCDDA 2014">{{Cite report|url=http://www.emcdda.europa.eu/attachements.cfm/att_228272_EN_TDAT14001ENN.pdf|title=European drug report 2014: Trends and developments|last=European Monitoring Centre for Drugs Drug Addiction|date=May 2014|publisher=European Monitoring Centre for Drugs and Drug Addiction|doi=10.2810/32306|location=Lisbon, Portugal|pages=13, 24|issn=2314-9086|quote=1.2 million or 0.9% of young adults (15–34) used amphetamines in the last year|access-date=18 August 2014|archive-url=https://ghostarchive.org/archive/20221009/http://www.emcdda.europa.eu/attachements.cfm/att_228272_EN_TDAT14001ENN.pdf|archive-date=2022-10-09}}</ref> "Giá bán trên đường phố" amphetamin bất hợp pháp trong EU dao động từ {{Nowrap|6–38 [[Euro|€]]}} mỗi gam (khoảng 170.000 đến 1.070.000 đồng, theo tỷ giá EUR-VND năm 2014).<ref name="EMCDDA 2014" /> Bên ngoài châu Âu, thị trường chợ đen chất amphetamin nhỏ hơn nhiều so với thị trường methamphetamin và MDMA.<ref name="WDR2014" /> |
|||
=== Tình trạng pháp lý === |
|||
Theo kết quả của Công ước [[Liên Hợp Quốc|Liên hợp quốc]] năm 1971 về các chất hướng thần, amphetamin đã trở thành chất bị kiểm soát ở tất cả 183 quốc gia thành viên.<ref name="UN Convention">{{Chú thích web|url=http://treaties.un.org/Pages/ViewDetails.aspx?src=TREATY&mtdsg_no=VI-16&chapter=6&lang=en|tựa đề=Convention on psychotropic substances|website=United Nations Treaty Collection|nhà xuất bản=United Nations|url lưu trữ=https://web.archive.org/web/20160331074842/https://treaties.un.org/pages/ViewDetails.aspx?src=TREATY&mtdsg_no=VI-16&chapter=6&lang=en|ngày lưu trữ=31 March 2016|url-status=live|ngày truy cập=11 November 2013}}</ref> Do đó, amphetamin được quản lý chặt chẽ ở hầu hết các quốc gia.<ref name="UNODC2007">{{Chú thích sách|url=http://www.unodc.org/pdf/youthnet/ATS.pdf|title=Preventing Amphetamine-type Stimulant Use Among Young People: A Policy and Programming Guide|last=United Nations Office on Drugs and Crime|publisher=United Nations|year=2007|isbn=9789211482232|location=New York, USA|access-date=11 November 2013}}</ref><ref>{{Chú thích web|url=http://www.incb.org/pdf/e/list/green.pdf|tựa đề=List of psychotropic substances under international control|ngày=August 2003|website=International Narcotics Control Board|nhà xuất bản=United Nations|url lưu trữ=https://web.archive.org/web/20051205125434/http://www.incb.org/pdf/e/list/green.pdf|ngày lưu trữ=5 December 2005|ngày truy cập=19 November 2005}}</ref> Một số quốc gia, chẳng hạn như Hàn Quốc và Nhật Bản, đã cấm amphetamin thay thế ngay cả khi sử dụng chất trong y tế.<ref name="urlMoving to Korea brings medical, social changes">{{Chú thích web|url=https://www.koreatimes.co.kr/www/news/nation/2012/10/319_111757.html|tựa đề=Moving to Korea brings medical, social changes|tác giả=Park Jin-seng|ngày=25 May 2012|website=The Korean Times|ngày truy cập=14 November 2013}}</ref><ref>{{Chú thích web|url=http://www.mhlw.go.jp/english/topics/import/|tựa đề=Importing or Bringing Medication into Japan for Personal Use|ngày=1 April 2004|website=Japanese Ministry of Health, Labour and Welfare|ngày truy cập=3 November 2013}}</ref> Ở các quốc gia khác, chẳng hạn như Canada,<ref name="Canada Control">{{Chú thích web|url=http://laws-lois.justice.gc.ca/eng/acts/C-38.8/page-24.html#h-28|tựa đề=Controlled Drugs and Substances Act|website=Canadian Justice Laws Website|nhà xuất bản=Government of Canada|url lưu trữ=https://web.archive.org/web/20131122143804/http://laws-lois.justice.gc.ca/eng/acts/C-38.8/page-24.html|ngày lưu trữ=22 November 2013|ngày truy cập=11 November 2013}}</ref> Hà Lan,<ref name="Opiumwet">{{Chú thích web|url=http://wetten.overheid.nl/BWBR0001941/geldigheidsdatum_03-08-2009|tựa đề=Opiumwet|nhà xuất bản=Government of the Netherlands|ngày truy cập=3 April 2015}}</ref> Hoa Kỳ,<ref name="FDA">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=aff45863-ffe1-4d4f-8acf-c7081512a6c0|tựa đề=Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release|ngày=17 July 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref> Úc,<ref>{{Chú thích bách khoa toàn thư|title=Poisons Standard|publisher=Australian Government Department of Health|url=https://www.comlaw.gov.au/Details/F2015L01534/Html/Text|access-date=15 December 2015|date=October 2015}}</ref> Thái Lan,<ref>{{Chú thích web|url=http://narcotic.fda.moph.go.th/faq/upload/Thai%20Narcotic%20Act%202012.doc._37ef.pdf|tựa đề=Table of controlled Narcotic Drugs under the Thai Narcotics Act|ngày=22 May 2013|website=Thailand Food and Drug Administration|url lưu trữ=https://web.archive.org/web/20140308001155/http://narcotic.fda.moph.go.th/faq/upload/Thai%20Narcotic%20Act%202012.doc._37ef.pdf|ngày lưu trữ=8 March 2014|ngày truy cập=11 November 2013}}</ref> và Vương quốc Anh,<ref>{{Chú thích web|url=http://www.homeoffice.gov.uk/drugs/drugs-law/Class-a-b-c/|tựa đề=Class A, B and C drugs|website=Home Office, Government of the United Kingdom|url lưu trữ=https://web.archive.org/web/20070804233232/http://www.homeoffice.gov.uk/drugs/drugs-law/Class-a-b-c/|ngày lưu trữ=4 August 2007|ngày truy cập=23 July 2007}}</ref> amphetamin nằm trong mục thuốc bị kiểm soát trong dược thư quốc gia, vẫn được cho phép sử dụng để điều trị y tế.<ref name="WDR2014">{{Chú thích web|url=https://www.unodc.org/documents/wdr2014/World_Drug_Report_2014_web.pdf|tựa đề=World Drug Report 2014|ngày=June 2014|editor=Mohan J|website=United Nations Office on Drugs and Crime|trang=3|ngày truy cập=18 August 2014}}</ref> |
|||
=== Dược phẩm === |
|||
Một số công thức amphetamin được bán trên thị trường hiện có chứa cả hai đối quang, gồm Adderall, Adderall XR, Mydayis, Adzenys ER, {{Nowrap|Adzenys XR-ODT}}, Dyanavel XR, Evekeo và Evekeo ODT. Trong đó, Evekeo (bao gồm Evekeo ODT) là sản phẩm duy nhất chỉ chứa racemic amphetamin (như amphetamin sulfat), và do đó đây là sản phẩm duy nhất có nhóm chức hoạt động của "amphetamin".<ref name="Stahl's Essential Psychopharmacology">{{Chú thích sách|title=Prescriber's Guide: Stahl's Essential Psychopharmacology|vauthors=Stahl SM|date=March 2017|publisher=Cambridge University Press|isbn=9781108228749|edition=6th|location=Cambridge, United Kingdom|pages=45–51|chapter=Amphetamine (D,L)|access-date=5 August 2017|chapter-url=https://books.google.com/books?id=9hssDwAAQBAJ&pg=PA45}}</ref><ref name="Evekeo">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f469fb38-0380-4621-9db3-a4f429126156|tựa đề=Evekeo- amphetamine sulfate tablet|ngày=14 August 2019|website=DailyMed|nhà xuất bản=Arbor Pharmaceuticals, LLC|ngày truy cập=22 December 2019}}</ref> Dextroamphetamin, được bán trên thị trường dưới tên thương hiệu Dexedrine và Zenzedi, là sản phẩm amphetamin dạng [[Thuốc enantiopure|enantiopure]] (đối quang tinh khiết) duy nhất hiện có. Một [[Tiền chất|dạng tiền chất]] của dextroamphetamin là [[lisdexamfetamine|lisdexamfetamin]] được bày bán trên thị trường dưới tên thương hiệu Vyvanse. Vì là một tiền chất, lisdexamfetamin có cấu trúc khác với dextroamphetamin và không hoạt động cho đến khi thuốc được chuyển hóa thành dextroamphetamin.<ref name="USVyvanselabel"><templatestyles src="Module:Citation/CS1/styles.css"></templatestyles><cite class="citation web cs1">[https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=704e4378-ca83-445c-8b45-3cfa51c1ecad "Vyvanse- lisdexamfetamine dimesylate capsule Vyvanse- lisdexamfetamine dimesylate tablet, chewable"]. ''DailyMed''. Shire US Inc. 30 October 2019<span class="reference-accessdate">. Retrieved<span class="nowrap">22 December</span> 2019</span>.</cite></ref> Racemic amphetamin trước đây mang tên thương mại là Benzedrine, Psychedrine và Sympatedrine.<ref name="Amph Uses">{{Chú thích tập san học thuật |vauthors=Heal DJ, Smith SL, Gosden J, Nutt DJ |date=June 2013 |title=Amphetamine, past and present – a pharmacological and clinical perspective |journal=Journal of Psychopharmacology |volume=27 |issue=6 |pages=479–496 |doi=10.1177/0269881113482532 |pmc=3666194 |pmid=23539642 |quote=The intravenous use of d-amphetamine and other stimulants still pose major safety risks to the individuals indulging in this practice. Some of this intravenous abuse is derived from the diversion of ampoules of d-amphetamine, which are still occasionally prescribed in the UK for the control of severe narcolepsy and other disorders of excessive sedation. ... For these reasons, observations of dependence and abuse of prescription d-amphetamine are rare in clinical practice, and this stimulant can even be prescribed to people with a history of drug abuse provided certain controls, such as daily pick-ups of prescriptions, are put in place (Jasinski and Krishnan, 2009b).}}</ref> Levoamphetamin trước đây có tên thương mại là Cydril.<ref name="Amph Uses" /> Nhiều dược phẩm amphetamin hiện tại là [[Muối (hóa học)|muối]] do khi ở dạng base tự do, thuốc có tính bay hơi tương đối cao.<ref name="Amph Uses" /> Tuy nhiên, [[dạng bào chế]] [[hỗn dịch uống]] và [[viên nén rã]] (ODT) chứa dạng base tư do của thuốc được giới thiệu năm 2015 và 2016.<ref name="FDA Dyanavel approval date">{{Chú thích web|url=https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/208147Orig1DyanavelTOC.cfm|tựa đề=Drug Approval Package: Amphetamine (Amphetamine)|website=United States Food and Drug Administration|ngày truy cập=22 December 2019}}</ref><ref name="Adzenys">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=c1179269-00b5-48ea-972d-31e614e99b7e|tựa đề=Adzenys XR-ODT- amphetamine tablet, orally disintegrating|ngày=9 February 2018|website=DailyMed|nhà xuất bản=Neos Therapeutics, Inc.|ngày truy cập=22 December 2019|trích dẫn=ADZENYS XR-ODT (amphetamine extended-release orally disintegrating tablet) contains a 3 to 1 ratio of d- to l-amphetamine, a central nervous system stimulant.}}</ref> Sau đây là một số tên thương mại của thuốc và thành phần của chúng. |
|||
{| class="wikitable sortable" style="text-align:center;" |
|||
|+Dược phẩm amphetamin |
|||
! scope="col" |Tên thương mại |
|||
! scope="col" |Hoạt chất |
|||
! class="unsortable" scope="col" style="text-align:center" | Tỷ lệ đối quang |
|||
[[wiktionary:enantiomeric ratio|(D:L)]] |
|||
! scope="col" |Bào chế |
|||
! class="unsortable" scope="col" | Năm bắt đầu sản xuất |
|||
! class="unsortable" scope="col" | Dữ liệu tại Hoa Kỳ |
|||
! class="unsortable" scope="col" |<small>Nguồn</small> |
|||
|- |
|||
| Adderall |
|||
| - |
|||
| 3: 1 <small>(muối)</small> |
|||
| viên nén |
|||
| 1996 |
|||
| [https://www.goodrx.com/adderall GoodRx] |
|||
|<ref name="Amph Uses">{{Chú thích tập san học thuật |vauthors=Heal DJ, Smith SL, Gosden J, Nutt DJ |date=June 2013 |title=Amphetamine, past and present – a pharmacological and clinical perspective |journal=Journal of Psychopharmacology |volume=27 |issue=6 |pages=479–496 |doi=10.1177/0269881113482532 |pmc=3666194 |pmid=23539642 |quote=The intravenous use of d-amphetamine and other stimulants still pose major safety risks to the individuals indulging in this practice. Some of this intravenous abuse is derived from the diversion of ampoules of d-amphetamine, which are still occasionally prescribed in the UK for the control of severe narcolepsy and other disorders of excessive sedation. ... For these reasons, observations of dependence and abuse of prescription d-amphetamine are rare in clinical practice, and this stimulant can even be prescribed to people with a history of drug abuse provided certain controls, such as daily pick-ups of prescriptions, are put in place (Jasinski and Krishnan, 2009b).}}</ref> |
|||
|- |
|||
| Adderall XR |
|||
| - |
|||
| 3: 1 <small>(muối)</small> |
|||
| viên con nhộng |
|||
| 2001 |
|||
| [https://www.goodrx.com/adderall-xr GoodRx] |
|||
|<ref name="Amph Uses" /> |
|||
|- |
|||
| Mydayis |
|||
| - |
|||
| 3: 1 <small>(muối)</small> |
|||
| viên con nhộng |
|||
| 2017 |
|||
| [https://www.goodrx.com/mydayis GoodRx] |
|||
|<ref name="Mydayis">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=141a7970-3f06-44ea-9ab7-aeece2c085fc|tựa đề=Mydayis- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate capsule, extended release|ngày=11 October 2019|website=DailyMed|nhà xuất bản=Shire US Inc.|ngày truy cập=22 December 2019}}</ref><ref>{{Chú thích web|url=https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/022063Orig1s000TOC.cfm|tựa đề=Drug Approval Package: Mydayis (mixed salts of a single-entity amphetamine product)|ngày=6 June 2018|website=United States Food and Drug Administration|ngày truy cập=22 December 2019}}</ref> |
|||
|- |
|||
| Adzenys ER |
|||
| amphetamin |
|||
| 3: 1 <small>(base)</small> |
|||
| hỗn dịch uống |
|||
| 2017 |
|||
| [https://www.goodrx.com/adzenys-er GoodRx] |
|||
|<ref name="Adzenys ER">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=eb1cc8d0-4231-41ea-8535-4fd872129713|tựa đề=Adzenys ER- amphetamine suspension, extended release|ngày=8 December 2017|website=DailyMed|nhà xuất bản=Neos Therapeutics, Inc.|ngày truy cập=25 December 2019}}</ref> |
|||
|- |
|||
| {{Nowrap|Adzenys XR-ODT}} |
|||
| amphetamin |
|||
| 3: 1 <small>(base)</small> |
|||
| viên nén rã |
|||
| 2016 |
|||
| [https://www.goodrx.com/adzenys-xr-odt GoodRx] |
|||
|<ref name="Adzenys">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=c1179269-00b5-48ea-972d-31e614e99b7e|tựa đề=Adzenys XR-ODT- amphetamine tablet, orally disintegrating|ngày=9 February 2018|website=DailyMed|nhà xuất bản=Neos Therapeutics, Inc.|ngày truy cập=22 December 2019|trích dẫn=ADZENYS XR-ODT (amphetamine extended-release orally disintegrating tablet) contains a 3 to 1 ratio of d- to l-amphetamine, a central nervous system stimulant.}}</ref><ref name="FDA Adzenys approval date">{{Chú thích web|url=https://www.accessdata.fda.gov/drugsatfda_docs/nda/2016/204326Orig1_toc.cfm|tựa đề=Drug Approval Package: Adzenys XR-ODT (amphetamine)|website=United States Food and Drug Administration|ngày truy cập=22 December 2019}}</ref> |
|||
|- |
|||
| Dyanavel XR |
|||
| amphetamin |
|||
| 3,2: 1 <small>(base)</small> |
|||
| hỗn dịch uống |
|||
| 2015 |
|||
| [https://www.goodrx.com/dyanavel-xr GoodRx] |
|||
|<ref name="FDA Dyanavel approval date">{{Chú thích web|url=https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/208147Orig1DyanavelTOC.cfm|tựa đề=Drug Approval Package: Amphetamine (Amphetamine)|website=United States Food and Drug Administration|ngày truy cập=22 December 2019}}</ref> |
|||
|- |
|||
| Evekeo |
|||
| amphetamin sulfat |
|||
| 1: 1 <small>(muối)</small> |
|||
| viên nén |
|||
| 2012 |
|||
| [https://www.goodrx.com/evekeo GoodRx] |
|||
|<ref name="Evekeo">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f469fb38-0380-4621-9db3-a4f429126156|tựa đề=Evekeo- amphetamine sulfate tablet|ngày=14 August 2019|website=DailyMed|nhà xuất bản=Arbor Pharmaceuticals, LLC|ngày truy cập=22 December 2019}}</ref><ref name="Racemic amph - FDA Evekeo status">{{Chú thích web|url=https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&applno=200166|tựa đề=Evekeo|website=United States Food and Drug Administration|ngày truy cập=11 August 2015}}</ref> |
|||
|- |
|||
| Evekeo ODT |
|||
| amphetamin sulfat |
|||
| 1: 1 <small>(muối)</small> |
|||
| viên nén rã |
|||
| 2019 |
|||
| [https://www.goodrx.com/evekeo?dosage=10mg&form=orally-disintegrating-tab&label_override=Evekeo&quantity=60 GoodRx] |
|||
|<ref name="Evekeo ODT">{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=1e25f905-6c0b-4b19-a3b6-b2a386afa1c3|tựa đề=Evekeo ODT- amphetamine sulfate tablet, orally disintegrating|ngày=7 June 2019|website=DailyMed|nhà xuất bản=Arbor Pharmaceuticals, LLC|ngày truy cập=25 December 2019}}</ref> |
|||
|- |
|||
| Dexedrine |
|||
| dextroamphetamin sulfat |
|||
| 1: 0 <small>(muối)</small> |
|||
| viên con nhộng |
|||
| Năm 1976 |
|||
| [https://www.goodrx.com/dexedrine-spansule GoodRx] |
|||
|<ref name="Amph Uses" /> |
|||
|- |
|||
| Zenzedi |
|||
| dextroamphetamin sulfat |
|||
| 1: 0 <small>(muối)</small> |
|||
| viên nén |
|||
| 2013 |
|||
| [https://www.goodrx.com/zenzedi GoodRx] |
|||
|<ref>{{Chú thích web|url=https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=d6394df5-f2c9-47eb-b57e-f3e9cfd94f84|tựa đề=Zenzedi- dextroamphetamine sulfate tablet|ngày=14 August 2019|website=DailyMed|nhà xuất bản=Arbor Pharmaceuticals, LLC|ngày truy cập=22 December 2019}}</ref> |
|||
|- |
|||
| rowspan="2" | Vyvanse |
|||
| rowspan="2" | lisdexamfetamin dimesylate |
|||
| rowspan="2" | 1: 0 <small>(tiền chất)</small> |
|||
| viên con nhộng |
|||
| rowspan="2" | 2007 |
|||
| rowspan="2" | [https://www.goodrx.com/vyvanse GoodRx] |
|||
| rowspan="2" |<ref name="Amph Uses">{{Chú thích tập san học thuật |vauthors=Heal DJ, Smith SL, Gosden J, Nutt DJ |date=June 2013 |title=Amphetamine, past and present – a pharmacological and clinical perspective |journal=Journal of Psychopharmacology |volume=27 |issue=6 |pages=479–496 |doi=10.1177/0269881113482532 |pmc=3666194 |pmid=23539642 |quote=The intravenous use of d-amphetamine and other stimulants still pose major safety risks to the individuals indulging in this practice. Some of this intravenous abuse is derived from the diversion of ampoules of d-amphetamine, which are still occasionally prescribed in the UK for the control of severe narcolepsy and other disorders of excessive sedation. ... For these reasons, observations of dependence and abuse of prescription d-amphetamine are rare in clinical practice, and this stimulant can even be prescribed to people with a history of drug abuse provided certain controls, such as daily pick-ups of prescriptions, are put in place (Jasinski and Krishnan, 2009b).}}<cite class="citation journal cs1" data-ve-ignore="true" id="CITEREFHealSmithGosdenNutt2013">Heal DJ, Smith SL, Gosden J, Nutt DJ (June 2013). [//www.ncbi.nlm.nih.gov/pmc/articles/PMC3666194 "Amphetamine, past and present – a pharmacological and clinical perspective"]. ''Journal of Psychopharmacology''. '''27''' (6): 479–496. [[DOI|doi]]:[[doi:10.1177/0269881113482532|10.1177/0269881113482532]]. [[PubMed Central|PMC]] <span class="cs1-lock-free" title="Freely accessible">[//www.ncbi.nlm.nih.gov/pmc/articles/PMC3666194 3666194]</span>. [[PubMed|PMID]] [//pubmed.ncbi.nlm.nih.gov/23539642 23539642].<q>The intravenous use of d-amphetamine and other stimulants still pose major safety risks to the individuals indulging in this practice. Some of this intravenous abuse is derived from the diversion of ampoules of d-amphetamine, which are still occasionally prescribed in the UK for the control of severe narcolepsy and other disorders of excessive sedation. ... For these reasons, observations of dependence and abuse of prescription d-amphetamine are rare in clinical practice, and this stimulant can even be prescribed to people with a history of drug abuse provided certain controls, such as daily pick-ups of prescriptions, are put in place (Jasinski and Krishnan, 2009b).</q></cite></ref><ref name="USVyvanselabel"><templatestyles src="Module:Citation/CS1/styles.css"></templatestyles><cite class="citation web cs1">[https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=704e4378-ca83-445c-8b45-3cfa51c1ecad "Vyvanse- lisdexamfetamine dimesylate capsule Vyvanse- lisdexamfetamine dimesylate tablet, chewable"]. ''DailyMed''. Shire US Inc. 30 October 2019<span class="reference-accessdate">. Retrieved<span class="nowrap">22 December</span> 2019</span>.</cite></ref><ref>{{Chú thích web|url=https://www.accessdata.fda.gov/drugsatfda_docs/nda/2007/021977s000TOC.cfm|tựa đề=Drug Approval Package: Vyvanse (Lisdexamfetamine Dimesylate) NDA #021977|ngày=24 December 1999|website=United States Food and Drug Administration|ngày truy cập=22 December 2019}}</ref> |
|||
|- |
|||
| viên nén |
|||
|- |
|||
| Xelstrym |
|||
| dextroamphetamin |
|||
| 1: 0 <small>(base)</small> |
|||
| thuốc dán |
|||
| 2022 |
|||
| [https://www.goodrx.com/xelstrym GoodRx] |
|||
|<ref name="US-Xelstrym-Label">{{Chú thích web|url=https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215401s000lbl.pdf|tựa đề=Approval [Rx ONLY]|website=U.S. Food and Drug Administration|url-status=live|ngày truy cập=11 October 2022}}</ref> |
|||
|} |
|||
[[Thể loại:Chất bị Cơ quan phòng chống doping thế giới cấm]] |
|||
[[Thể loại:Amphetamin]] |
|||
[[Thể loại:Chất kích thích]] |
[[Thể loại:Chất kích thích]] |
||
[[Thể loại:Amphetamin| ]] |
|||
[[Thể loại:Phát minh của Đức]] |
|||
[[Thể loại:Phenethylamin]] |
[[Thể loại:Phenethylamin]] |
||
[[Thể loại: |
[[Thể loại:Phát minh của Đức]] |
||
[[Thể loại: |
[[Thể loại:Thuốc trong thể thao]] |
||
[[Thể loại:Thuốc tác động lên hệ thần kinh]] |
|||
[[Thể loại:Thuốc tác động lên hệ tim mạch]] |
|||
[[Thể loại:Nguồn CS1 tiếng Nhật (ja)]] |
|||
[[Thể loại:Bài viết sử dụng định dạng hAudio]] |
|||
Phiên bản lúc 15:52, ngày 24 tháng 10 năm 2022
 | |
 | |
| Dữ liệu lâm sàng | |
|---|---|
| Phát âm | /æmˈfɛtəmiːn/ ⓘ |
| Tên thương mại | Evekeo, Adderall,[note 1] others |
| Đồng nghĩa | α-methylphenethylamine |
| AHFS/Drugs.com | Chuyên khảo |
| MedlinePlus | a616004 |
| Giấy phép |
|
| Nguy cơ lệ thuộc | Moderate[1] |
| Nguy cơ gây nghiện | Moderate |
| Dược đồ sử dụng | Medical: oral, intravenous[2] Recreational: oral, insufflation, rectal, intravenous, intramuscular |
| Mã ATC | |
| Tình trạng pháp lý | |
| Tình trạng pháp lý |
|
| Dữ liệu dược động học | |
| Sinh khả dụng | Oral: 75–100%[8] |
| Liên kết protein huyết tương | 20%[9] |
| Chuyển hóa dược phẩm | CYP2D6,[3] DBH,[4][5] FMO3[4][6][7] |
| Chất chuyển hóa | 4-hydroxyamphetamine, 4-hydroxynorephedrine, 4-hydroxyphenylacetone, benzoic acid, hippuric acid, norephedrine, phenylacetone[3][10] |
| Bắt đầu tác dụng | IR dosing: 30–60 minutes[11] XR dosing: 1.5–2 hours[12][13] |
| Chu kỳ bán rã sinh học | D-amph: 9–11 hours[3][14] L-amph: 11–14 hours[3][14] pH-dependent: 7–34 hours[15] |
| Thời gian hoạt động | IR dosing: 3–6 hours[1][12][16] XR dosing: 8–12 hours[1][12][16] |
| Bài tiết | Primarily renal; pH-dependent range: 1–75%[3] |
| Các định danh | |
Tên IUPAC
| |
| Số đăng ký CAS | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| Định danh thành phần duy nhất | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| NIAID ChemDB | |
| ECHA InfoCard | 100.005.543 |
| Dữ liệu hóa lý | |
| Công thức hóa học | C9H13N |
| Khối lượng phân tử | 135,21 g·mol−1 |
| Mẫu 3D (Jmol) | |
| Tỉ trọng | .936 g/cm3 at 25 °C[17] |
| Điểm nóng chảy | 11,3 °C (52,3 °F) (predicted)[18] |
| Điểm sôi | 203 °C (397 °F) at 760 mmHg[19] |
SMILES
| |
Định danh hóa học quốc tế
| |
| (kiểm chứng) | |
Amphetamin (hay còn gọi là hồng phiến,[20] viết tắt của alpha-methylphenethylamin, danh pháp theo tiếng Anh là Amphetamin) là một chất kích thích hệ thần kinh trung ương (TKTW) mạnh được sử dụng trong điều trị rối loạn tăng động giảm chú ý (ADHD), chứng ngủ rũ và béo phì. Amphetamin được phát hiện vào năm 1887 và tồn tại dưới dạng hai chất đối quang (enantiomer): levoamphetamin và dextroamphetamin. Danh pháp amphetamin đề cập đến hỗn hợp racemic chứa hai đồng phân đối quang ở dạng amin tinh khiết với tỷ lệ ngang nhau. Danh pháp này thường được sử dụng để chỉ hoặc là hỗn hợp hai chất đối quang, hoặc là chỉ một trong hai chất nêu trên. Cách dùng trên là quy ước không chính thức. Trong lịch sử, amphetamin được sử dụng để điều trị nghẹt mũi và trầm cảm. Amphetamin cũng được sử dụng là chất cải thiện khả năng thi đấu trong thể thao, thuốc hưng trí, thuốc kích dục và thuốc làm tăng hưng phấn. Amphetamin là thuốc theo toa ở nhiều quốc gia, và việc sở hữu và phân phối amphetamin được kiểm soát chặt chẽ do những nguy cơ to lớn của thuốc lên sức khỏe nếu việc sử dụng thuốc phục vụ mục đích giải trí. [sources 1]
Dược phẩm chứa hoạt chất amphetamin đầu tiên là Benzedrine, được chỉ định để điều trị nhiều loại bệnh. Hiện tại, các thành phẩm amphetamin làm dược phẩm được kê đơn bao gồm: hỗn hợp racemic amphetamin, thuốc Adderall, [note 2] thuốc dextroamphetamin, hoặc tiền chất không hoạt tính lisdexamfetamin . Amphetamin làm tăng số lượng và kích thích tiết chất dẫn truyền thần kinh monoamin trong não, với tác dụng rõ rệt nhất là nhắm vào hệ thống dẫn truyền thần kinh noradrenalin và dopamin.[sources 2]
Về mặt y học, ở liều điều trị, amphetamin gây ra các hiệu ứng về cảm xúc và nhận thức như hưng phấn, thay đổi ham muốn tình dục, tăng tỉnh táo và cải thiện khả năng kiểm soát nhận thức. Chất tác động về mặt thể chất như cải thiện thời gian đáp ứng, chống mệt mỏi và tăng sức mạnh cơ bắp. Liều amphetamin lớn hơn có thể làm suy giảm chức năng nhận thức và gây ra tiêu cơ vân. Nghiện là một tình trạng nghiêm trọng khi lạm dụng amphetamin để giải trí, nhưng ít có khả năng nghiện nếu sử dụng chất ở liều điều trị trong các cơ sở y tế. Liều rất cao có thể dẫn đến rối loạn tâm thần do chất kích thích (ví dụ, hoang tưởng (delusion) và tâm thần phân liệt thể paranoid), những rối loạn tâm thần này hiếm khi xảy ra ở liều điều trị ngay cả khi sử dụng lâu dài. Liều giải trí nói chung lớn hơn nhiều so với liều điều trị được chỉ định và có nguy cơ tác dụng phụ nghiêm trọng cao hơn nhiều.[sources 3]
Về mặt hóa học, amphetamin thuộc lớp phenethylamine. Đây là hợp chất gốc của lớp cấu trúc riêng mang tên amphetamin thay thế, bao gồm các chất được biết đến nhiều như bupropion, cathinon, MDMA (thuốc lắc) và methamphetamin (ice, ma túy đá). Là một chất thuộc lớp phenethylamine, amphetamin cũng có liên quan về mặt hóa học với các chất điều biến thần kinh (neuromodulator) trace amine (là chất chủ vận TAAR1), cụ thể là phenethylamine và N-methylphenethylamine, cả hai đều được sản xuất trong cơ thể con người. Phenethylamine là hợp chất gốc của amphetamin, trong khi N-methylphenethylamine là đồng phân cấu tạo của amphetamin, chỉ khác nhau ở vị trí của nhóm methyl.
Ứng dụng
Y học
Amphetamin được sử dụng để điều trị rối loạn tăng động giảm chú ý (ADHD), chứng ngủ rũ (rối loạn giấc ngủ) và béo phì, và đôi khi được kê đơn off-label (kê đơn không theo hướng dẫn trên nhãn) cho các chỉ định trước đây, đặc biệt là đối với trầm cảm kháng trị (trầm cảm không đáp ứng với thuốc) và đau mạn tính.[1][31][42] Phơi nhiễm với amphetamin lâu dài với liều lượng đủ cao ở một số loài động vật được cho là gây ra sự phát triển bất thường của hệ dopamine hoặc tổn thương thần kinh,[43][44] nhưng ở người bị ADHD, amphetamin dược phẩm ở liều lượng điều trị dường như cải thiện sự phát triển của não và tăng trưởng thần kinh.[45][46][47] Đánh giá các nghiên cứu chụp cộng hưởng từ (MRI) cho thấy rằng điều trị lâu dài với amphetamin làm giảm các bất thường trong cấu trúc và chức năng não ở những đối tượng mắc ADHD, và cải thiện chức năng ở một số phần của não, chẳng hạn như nhân đuôi phải của hạch nền.[45][46][47]
Các đánh giá về nghiên cứu chất kích thích trên lâm sàng đã xác định tính an toàn và hiệu quả của việc sử dụng amphetamin liên tục trong thời gian dài để điều trị ADHD.[39][48][49] Các thử nghiệm ngẫu nhiên có đối chứng về liệu pháp kích thích liên tục để điều trị ADHD kéo dài 2 năm đã chứng minh hiệu quả điều trị và độ an toàn.[39][48] Hai đánh giá đã chỉ ra rằng liệu pháp kích thích liên tục trong thời gian dài ở bệnh nhân ADHD có hiệu quả để giảm các triệu chứng chủ đạo của ADHD (gồm tăng động, giảm chú ý và xung động), nâng cao chất lượng cuộc sống và thành tích học tập, đồng thời cải thiện phần lớn các kết quả chức năng[note 3] dựa trên kết quả của 9 lĩnh vực, bao gồm: học vấn, hành vi chống đối xã hội, lái xe, sử dụng thuốc tùy tiện, béo phì, nghề nghiệp, lòng tự trọng, sử dụng dịch vụ (tức là các dịch vụ về học tập, nghề nghiệp, sức khỏe, tài chính và pháp lý) và chức năng xã hội.[39][49] Một thử nghiệm ngẫu nhiên có đối chứng kéo dài 9 tháng về điều trị bằng amphetamin cho ADHD ở trẻ em đã phát hiện ra mức tăng trung bình là 4,5 điểm IQ, cải thiện khả năng tập trung và tiếp tục giảm các hành vi gây rối và tăng động.[48] Một đánh giá khác chỉ ra rằng, dựa trên các nghiên cứu thuần tập có thời gian theo dõi dài nhất cho đến hiện tại, liệu pháp kích thích bắt đầu thực hiện từ lúc còn là trẻ nhỏ liên tục có hiệu quả để kiểm soát các triệu chứng ADHD và giảm nguy cơ tiến triển thành rối loạn tâm thần do sử dụng chất gây nghiện khi trưởng thành.[39]
Các mô hình hiện tại của ADHD cho thấy rằng bệnh có liên quan đến sự suy giảm chức năng trong một số hệ thống dẫn truyền thần kinh của não.[50] Những suy giảm chức năng này liên quan đến suy giảm chất dẫn truyền thần kinh dopamine trong con đường dopaminergic và chất dẫn truyền thần kinh noradrenalin trong con đường noradrenergic từ nhân lục (locus coeruleus) đến vỏ não trước trán.[50] Các chất kích thích tâm lý như methylphenidate và amphetamin có hiệu quả trong điều trị ADHD vì chúng làm tăng hoạt động dẫn truyền thần kinh trong các hệ thống này.[22][50][51] Khoảng 80% những người sử dụng các chất kích thích nêu trên cho thấy các triệu chứng ADHD được cải thiện.[52] Trẻ ADHD sử dụng thuốc kích thích nói chung có mối quan hệ tốt hơn với bạn bè đồng trang lứa và các thành viên trong gia đình, học giỏi hơn ở trường, ít mất tập trung và xung động hơn, đồng thời có thời gian chú ý lâu hơn.[53][54] Trong tổng quan hệ thống của tổ chức Cochrane về việc điều trị ADHD ở trẻ em, thanh thiếu niên và người lớn bằng thuốc amphetamin cho thấy rằng các nghiên cứu thời gian ngắn đã chứng minh các loại thuốc này làm giảm mức độ nghiêm trọng của các triệu chứng, nhưng lại có tỷ lệ ngừng thuốc cao hơn so với các loại thuốc không gây kích thích do tác dụng phụ bất lợi của thuốc.[55][56] Tổng quan của Cochrane về điều trị ADHD ở trẻ em bị rối loạn tic như hội chứng Tourette chỉ ra rằng các chất kích thích nói chung không làm cho tic tồi tệ hơn, nhưng liều cao dextroamphetamin có thể làm trầm trọng thêm tic ở một số đối tượng.[57]
Cải thiện các chức năng
Cải thiện nhận thức
Năm 2015, một tổng quan hệ thống và phân tích tổng hợp các thử nghiệm lâm sàng cho thấy rằng, khi được sử dụng ở liều thấp (liều điều trị), amphetamin cải thiện mặc dù ít nhưng vẫn đáng kể trong nhận thức, bao gồm trí nhớ hoạt động (working memory), trí nhớ từng hồi dài hạn (long-term episodic memory), kiểm soát ức chế, và một số khía cạnh của sự chú ý ở người lớn khỏe mạnh bình thường;[58][59] Những tác dụng tăng cường nhận thức này của amphetamin là do cơ chế trung gian: amphetamin là chất chủ vận, kích hoạt gián tiếp đồng thời cả thụ thể dopamine D1 và thụ thể α2 adrenergic ở vỏ não trước trán.[22][58] Một tổng quan hệ thống năm 2014 cho thấy liều lượng amphetamin thấp cũng cải thiện khả năng củng cố trí nhớ, từ đó dẫn đến cải thiện khả năng nhớ lại thông tin (recall).[60] Liều điều trị của amphetamin cũng tăng cường hiệu quả dẫn truyền tại mạng lưới vỏ não, đây một tác dụng làm cải thiện trí nhớ hoạt động.[22][61] Amphetamin và các chất kích thích ADHD khác cũng cải thiện task saliency (tạm dịch: sự nổi bật của nhiệm vụ, thuật ngữ chỉ một quá trình nhận thức để giành sự tập trung chú ý để thúc đẩy, tạo động lực thực hiện và hoàn thành nhiệm vụ) và tăng tỉnh táo, từ đó thúc đẩy hành vi hướng đến mục tiêu đã đề ra.[22][62][63] Các chất kích thích như amphetamin có thể cải thiện hiệu suất trong các nhiệm vụ khó khăn và nhàm chán. Có một số sinh viên sử dụng chất như một biện pháp hỗ trợ trong học tập và làm bài kiểm tra.[22][63][64] Dựa trên các nghiên cứu về việc sử dụng chất kích thích bất hợp pháp tự báo cáo, 5–35% sinh viên đại học sử dụng chất kích thích chủ yếu được sử dụng để nâng cao thành tích học tập chứ không phải là để chơi bời, tiêu khiển.[65][66][67] Tuy nhiên, liều amphetamin cao trên liều điều trị có thể ảnh hưởng đến trí nhớ hoạt động và các khía cạnh khác của kiểm soát nhận thức.[22][63]
Cải thiện thể chất
Amphetamin được một số vận động viên sử dụng vì tác dụng cải thiện thể chất, chẳng hạn như tăng sức bền và sự tỉnh táo;[35] Tuy nhiên, các cơ quan chống doping của quốc gia và quốc tế đã cấm việc sử dụng amphetamin ngoài mục đích y tế tại các sự kiện thể thao.[68][69] Ở những người khỏe mạnh với liều điều trị bằng đường uống, amphetamin đã được chứng minh là làm tăng sức mạnh thể chất, tăng tốc độ di chuyển, cải thiện thể chất, hoạt động trong các bài tập kỵ khí (còn gọi là bài tập yếm khí) và bài tập sức bền (tức là thuốc làm trì hoãn sự mệt mỏi khi tập các bài tập này), đồng thời cải thiện thời gian đáp ứng (bằng cách đo thời gian tâm lý, mental chronometry).[70][71] Amphetamin cải thiện sức bền và thời gian đáp ứng chủ yếu thông qua ức chế tái hấp thu và giải phóng dopamine trong hệ TKTW.[70][71][72] Amphetamin và các loại thuốc dopaminergic khác cũng làm tăng nguồn năng lượng phục vụ cho hoạt động gắng sức bằng cách cho phép tăng ngưỡng thân nhiệt để đạt được khả năng hoạt động mà nếu không sử dụng thuốc thì đây là những hoạt động quá giới hạn, không thể làm được.[71][73][74] Ở liều điều trị, tác dụng phụ của amphetamin không ảnh hưởng đến hoạt động thể thao;[70] Tuy nhiên, ở liều lượng cao hơn nhiều lần liều điều trị, amphetamin có thể gây ra các tác động làm suy giảm thể chất nghiêm trọng do làm tiêu cơ vân (tức là phân hủy cơ) và tăng thân nhiệt.[24][70]
Chống chỉ định
Theo Chương trình Quốc tế về An toàn Hóa chất (IPCS) và Cục Quản lý Thực phẩm và Dược phẩm Hoa Kỳ (USFDA), [note 8] chống chỉ định amphetamin ở những người có tiền sử lạm dụng chất, bệnh tim mạch, kích động nặng, hoặc quá lo lắng.[31][24] Chất cũng được chống chỉ định ở những người bị xơ cứng động mạch, glôcôm (tăng nhãn áp), cường giáp (tiết quá nhiều hormone tuyến giáp), hoặc tăng huyết áp từ trung bình đến nặng.[31][24] Các tổ chức này chỉ ra rằng những người đã trải qua phản ứng quá mẫn với các chất kích thích khác, hoặc đang dùng chất ức chế monoamin oxidase (MAOI) không nên dùng amphetamin,[31][24] mặc dù việc sử dụng đồng thời amphetamin và chất ức chế monoamine oxidase đã được ghi nhận là an toàn.[75][76] Các tổ chức này cũng khuyến cáo rằng bất kỳ ai mắc chán ăn tâm thần, rối loạn lưỡng cực, trầm cảm, tăng huyết áp, chức năng gan hoặc thận bất thường, hưng cảm, loạn thần, hội chứng Raynaud, cơn động kinh, các vấn đề về tuyến giáp, tic hay hội chứng Tourette nên theo dõi các triệu chứng trong khi dùng amphetamin.[24] Bằng chứng từ các nghiên cứu trên người chỉ ra rằng việc sử dụng amphetamin điều trị không gây ra các bất thường về phát triển ở thai nhi hoặc trẻ sơ sinh (tức là amphetamin không gây quái thai ở người), nhưng lạm dụng amphetamin có thể gây ra rủi ro cho thai nhi. Amphetamin cũng đã được chứng minh là có khả năng đi vào sữa mẹ, vì vậy hai tổ chức IPCS và USFDA khuyên các bà mẹ tránh cho con bú khi sử dụng thuốc.[24] Do khả năng gây suy giảm tăng trưởng thể chất có hồi phục, USFDA khuyến nghị nên theo dõi chiều cao và cân nặng của trẻ em và thanh thiếu niên khi trẻ được kê toa một loại dược phẩm chứa amphetamin.[24]
Tác dụng phụ
Amphetamin có rất nhiều tác dụng phụ bất lợi và có tính đa dạng. Liều lượng amphetamin được sử dụng là yếu tố chính để xác định khả năng xảy ra và mức độ nghiêm trọng của các tác dụng phụ.[24][35] Các chế phẩm amphetamin như Adderall, Dexedrine, và các sản phẩm tương đương hiện được USFDA chấp thuận để sử dụng điều trị lâu dài.[24] Sử dụng amphetamin để giải trí thường có liều lượng lớn hơn nhiều so với liều điều trị, có nguy cơ gây tác dụng phụ nghiêm trọng hơn so với liều lượng được sử dụng cho mục đích điều trị.[35]
Về mặt thể chất
Tác dụng phụ trên tim mạch bao gồm tăng huyết áp hay tụt huyết áp do ngất phế vị (ngất do phản xạ thần kinh phế vị hay thần kinh lang thang), hội chứng Raynaud (giảm lưu lượng máu đến bàn tay và bàn chân), và nhịp tim nhanh.[24][35][77] Tác dụng phụ về tình dục ở nam giới gồm rối loạn cường dương: cương cứng thường xuyên hoặc cương cứng kéo dài.[24] Tác dụng phụ về đường tiêu hóa gồm đau bụng, táo bón, tiêu chảy và buồn nôn.[1][24] Tác dụng phụ về thể chất khác bao gồm chán ăn, mờ mắt, khô miệng, nghiến răng quá mức, chảy máu cam, đổ mồ hôi nhiều, viêm mũi do thuốc, giảm ngưỡng co giật, rối loạn tic (một dạng rối loạn vận động) và giảm cân. Các tác dụng phụ nguy hiểm về thể chất hiếm khi xảy ra khi dùng ở liều điều trị.[35]
Amphetamin kích thích trung tâm hô hấp ở hành não, làm thở nhanh và sâu hơn.[35] Ở người bình thường ở liều điều trị, tác dụng này thường ít để ý, nhưng ở bệnh nhân có tổn thương hô hấp, tác dụng trên có thể biểu hiện rõ.[35] Amphetamin cũng gây ra co thắt cơ vòng ở bàng quang, (cơ kiểm soát việc đi tiểu), có thể gây bí tiểu.[35] Tác dụng phụ này có thể hữu ích trong việc điều trị đái dầm và tiểu tiện không tự chủ.[35] không đoán trước được tác dụng của amphetamin trên đường tiêu hóa.[35] Amphetamin có thể làm giảm nhu động ruột (liên quan tới tốc độ di chuyển của thức ăn qua hệ tiêu hóa);[35] tuy nhiên, amphetamin có thể làm tăng nhu động khi làm giãn cơ trơn đường tiêu hóa.[35] Amphetamin cũng có tác dụng giảm đau nhẹ và có thể hiệp dồng với tác dụng giảm đau của nhóm opioid.[1][35]
Các nghiên cứu do USFDA ủy quyền từ năm 2011 ở trẻ em, trẻ vị thành niên và người lớn chỉ ra rằng không có mối liên quan giữa các biến cố tim mạch nghiêm trọng (đột tử, đau tim và đột quỵ) với việc sử dụng amphetamin hoặc các chất kích thích ADHD khác trong y tế. [sources 6] Tuy nhiên, dược phẩm amphetamin có chống chỉ định ở những người mắc bệnh tim mạch.
Về mặt tâm lý
Ở liều điều trị bình thường, các tác dụng phụ về mặt tâm lý phổ biến nhất của amphetamin gồm tăng cảnh giác, lo lắng, tăng độ tập trung, tính chủ động, tự tin và hòa đồng, thay đổi khí sắc (khí sắc tăng sau đó là khí sắc trầm mức độ nhẹ), mất ngủ, tỉnh táo và giảm cảm giác mệt mỏi.[24][35] Các tác dụng phụ ít phổ biến hơn bao gồm lo lắng, thay đổi ham muốn tình dục, tính cách mạnh mẽ, cáu kỉnh, hành vi lặp đi lặp lại hoặc ám ảnh và bồn chồn; những tác động này phụ thuộc vào tính cách cá nhân và trạng thái tinh thần hiện tại của bệnh nhân.[35] Có nguy cơ rối loạn tâm thần do amphetamin (ví dụ, hoang tưởng và tâm thần phân liệt thể paranoid).[24][37] Rối loạn tâm thần này cũng có thể xảy ra ở liều điều trị nếu thời gian điều trị lâu dài.[24][37][38] Theo USFDA, "không có bằng chứng hệ thống" cho thấy chất kích thích tạo ra hành vi hung hăng hoặc thù địch.[24]
Amphetamin cũng được chứng minh là tạo ra ưa thích nơi chốn có điều kiện (conditioned place preference)[78] ở bệnh nhân tuân theo liều điều trị,[55][79] có nghĩa là bệnh nhân thích dành thời gian đi đến những nơi trước đây họ sử dụng amphetamin tại đó.[79]
Rối loạn tăng cường
Nghiện
| Thuật ngữ về chứng nghiện và phụ thuộc[80][81][82][83] | |
|---|---|
| |
Bản mẫu:Transcription factor glossary
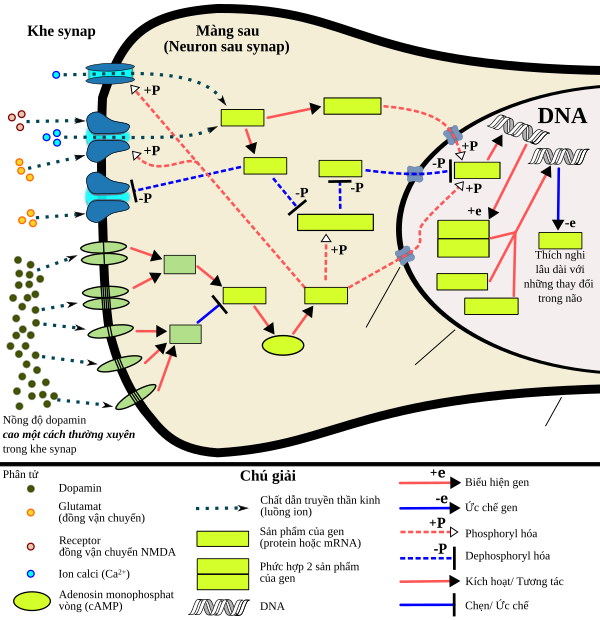
Nghiện là tác hại nghiêm trọng khi sử dụng amphetamin để giải trí, nhưng ít có khả năng xảy ra khi sử dụng lâu dài ở liều điều trị;[39][40][41] Trên thực tế, liệu pháp kích thích suốt đời đối với ADHD bắt đầu từ lúc còn nhỏ giúp giảm nguy cơ tiến triển thành mắc rối loạn tâm thần do sử dụng chất gây nghiện khi trưởng thành.[39] Con đường trung não-hồi viền (mesolimbic pathway, hay con đường phần thưởng) là con đường dopamine kết nối vùng mái não giữa (ventral tegmental area, VTA) với nhân cạp (nucleus accumbens, NAc). Sự hoạt động quá mức bệnh lý của con đường trung não-hồi viền trên đóng một vai trò trung tâm trong nghiện amphetamin.[91][92] Những người thường xuyên dùng amphetamin liều cao có nguy cơ cao bị nghiện amphetamin, vì việc sử dụng lâu dài ở liều cao dần dần làm tăng mức độ tích lũy protein ΔFosB tại nhân cạp, gây nên biểu hiện nghiện.[93][94] Một khi nhân cạp tích lũy ΔFosB được biểu hiện quá mức, mức độ nghiêm trọng của hành vi gây nghiện sẽ tăng dần (tức là người nghiện sẽ phải tự mình tìm ma túy).[93][95] Mặc dù hiện tại không có loại thuốc hiệu quả nào để điều trị nghiện amphetamin, việc tập các bài tập hiếu khí thường xuyên, liên tục dường như có thể làm giảm nguy cơ phát triển của nghiện.[96][97] Tập các bài tập hiếu khí thường xuyên liên tục có thể là một phương pháp điều trị hiệu quả cho người nghiện amphetamin. Liệu pháp tập thể dục cải thiện kết quả điều trị lâm sàng và có thể được sử dụng như một liệu pháp bổ trợ với các liệu pháp hành vi để điều trị nghiện.[96][98]
Cơ chế phân tử sinh học
Sử dụng amphetamin lâu ngày với liều lượng quá cao gây ra những thay đổi trong biểu hiện gen trong con đường trung não-hồi viền, phát sinh thông qua cơ chế phiên mã và di truyền học biểu sinh.[94][99][100] Các yếu tố phiên mã quan trọng nhất [note 11] tạo ra những thay đổi này là Delta FBJ murine osteosarcoma viral oncogene homolog B (ΔFosB), cAMP response element binding protein (CREB, tạm dịch: protein gắn yếu tố đáp ứng cAMP) và nuclear factor-kappa B (NF-κB, tạm dịch: Yếu tố hạt nhân tăng cường chuỗi nhẹ kappa của các tế bào B hoạt động).[94][101] ΔFosB là cơ chế phân tử sinh học quan trọng nhất trong chứng nghiện vì gen ΔFosB biểu hiện quá mức (tức là mức độ biểu hiện gen cao bất thường khi tạo ra kiểu hình) trong các neuron gai trung gian (medium spiny neurons) loại D1 trong nhân cạp (nucleus accumbens) là điều kiện cần và đủ [note 12] để có những thích ứng liên quan đến thần kinh và những sự điều chỉnh liên quan đến hành vi nghiện (ví dụ: tự tiêm chất gây nghiện theo chiều hướng tăng dần về liều).[93][94] Một khi ΔFosB được biểu hiện quá mức, ΔFosB gây ra trạng thái nghiện ngày càng nghiêm trọng hơn do chính những thích ứng liên quan đến thần kinh đó lại tiếp tục làm gia tăng hơn nữa sự biểu hiện quá mức của ΔFosB.[93] Cơ chế này có liên quan đến nghiện rượu, cannabinoid, cocain, methylphenidat, nicotin, opioid, phencyclidine, propofol và amphetamin thay thế, v..v.[source 10]
ΔJunD, một yếu tố phiên mã và G9a, một enzym histone methyltransferase, đều có tác dụng chống lại chức năng của ΔFosB và ức chế sự gia tăng biểu hiện gen của ΔFosB.[94][102] ΔJunD biểu hiện quá mức trong nhân cạp, phối hợp với vector virus (viral vector) có thể ngăn chặn hoàn toàn nhưng biến đổi liên quan đến thần kinh và hành vi được thấy trong lạm dụng chất lâu ngày (tức là những thay đổi qua trung gian là gen ΔFosB).[94] Tương tự, hiện tượng biểu hiện quá mức gen G9a tại nhân cạp làm tăng rõ rệt quá trình dimethyl hóa nhóm lysine dư thừa tại vị trí số 9 trên protein histon H3 (tiếng Anh: histone 3 lysine residue 9 dimethylation - H3K9me2, histon H3 là một protein đóng gói DNA) và ức chế sự cảm ứng của tính dẻo hành vi (behavioral plasticity) và khả biến thần kinh (neuroplasticity) qua trung gian ΔFosB do sử dụng thuốc dài ngày,[sources 11]. Sự ức chế trên xảy ra thông qua:[94][102]
- Ức chế qua trung gian H3K9me2 (H3K9me2-mediated repression) đối với các yếu tố phiên mã gen ΔFosB
- Ức chế qua trung gian H3K9me2 đối với các mục tiêu thúc đẩy sự phiên mã của gen ΔFosB (ví dụ: enzyme cyclin-dependent kinase 5, CDK5).
ΔFosB đóng vai trò quan trọng trong việc điều chỉnh các đáp ứng hành vi đối với hành vi nghiện, chẳng hạn như thưởng thức bữa ăn ngon, tình dục và tập thể dục.[95][94][103] Vì những "phần thưởng" nêu trên và thuốc gây nghiện đều gây ra biểu hiện gen của gen ΔFosB (tức là khiến não sản xuất ra nhiều hơn), việc lâu dài tiếp nhận các "phần thưởng" nêu trên cũng có thể dẫn đến tình trạng nghiện bệnh lý.[95][94] Do đó, ΔFosB là yếu tố quan trọng nhất liên quan đến cả nghiện amphetamin và nghiện tình dục do amphetamin, là những hành vi tình dục cưỡng bức do hoạt động tình dục quá mức và sử dụng amphetamin.[95][104][105] Những chứng nghiện tình dục này có liên quan đến hội chứng rối loạn điều hòa dopamin xảy ra ở một số bệnh nhân dùng thuốc dopaminergic.[95][103]
Tác dụng của amphetamin đối với sự điều hòa gen phụ thuộc vào liều lượng và đường dùng.[100] Hầu hết các nghiên cứu về điều hòa gen và nghiện đều dựa trên các nghiên cứu trên động vật, đều là những thí nghiệm amphetamin tiêm tĩnh mạch với liều rất cao.[100] Một vài nghiên cứu đã sử dụng liều điều trị tương đương (tức là liều được điều chỉnh theo cân nặng) ở người và dùng thuốc bằng đường uống cho thấy rằng những thay đổi trong điều hòa gen là tương đối nhỏ hoặc không có.[100] Như vậy, việc sử dụng amphetamin trong y tế không ảnh hưởng đáng kể đến sự điều hòa gen.[100]
Dược trị liệu (Liệu pháp hóa dược)
Tính đến tháng 12 năm 2019[cập nhật], chưa thấy hiệu quả của dược trị liệu (tức là điều trị dùng thuốc) cho bệnh nhân nghiện amphetamin.[106][107][108] Các tổng quan hệ thống từ năm 2015 và 2016 chỉ ra rằng chất đồng vận chọn lọc TAAR1 rất tiềm năng trong điều trị chứng nghiện chất kích thích tâm thần;[34][109] tuy nhiên, Tính đến tháng 2 năm 2016[cập nhật], các hợp chất có chức năng là chất chủ vận chọn lọc TAAR1 vẫn chỉ là thuốc thử nghiệm.[34][109] Nghiện amphetamin phần lớn qua thông qua sự gia tăng hoạt hóa các thụ thể dopamine và các thụ thể NMDA đồng khu trú [note 13] trong nhân cạp.[92] ion magnesi ức chế các receptor NMDA bằng cách chẹn receptor của kênh calci.[92] Một tổng quan hệ thống dựa trên thử nghiệm lên động vật khác cho thấy rằng, việc sử dụng chất kích thích tâm thần (chất gây nghiện) làm giảm đáng kể nồng độ magnesi nội bào trong não. Điều trị bổ sung magnesi [note 14] đã được chứng minh là làm giảm việc tự tiêm amphetamin ở người, nhưng đây không phải là hình thức đơn trị liệu hiệu quả cho bệnh nhân nghiện amphetamin.[92]
Một tổng quan hệ thống và phân tích tổng hợp từ năm 2019 đã đánh giá hiệu quả của 17 liệu pháp hóa dược khác nhau được sử dụng trong các thử nghiệm ngẫu nhiên có đối chứng đối với bệnh nhân nghiện amphetamin và methamphetamin.[107] Kết quả: chỉ tìm thấy bằng chứng mức độ thấp cho thấy methylphenidat có thể làm giảm việc người nghiện tự tiêm amphetamin hoặc methamphetamin.[107] Có bằng chứng mức thấp đến trung bình về việc hầu hết các thuốc khác được sử dụng trong các thử nghiệm nêu trên là không mang lại lợi ích, bao gồm thuốc chống trầm cảm (bupropion, mirtazapine, sertraline), thuốc chống loạn thần (aripiprazole), thuốc chống co giật (topiramate, baclofen, gabapentin), naltrexone, varenicline, citicoline, ondansetron, prometa, riluzole, atomoxetine, dextroamphetamin và modafinil.[107]
Liệu pháp tâm lý hành vi
Một tổng quan hệ thống năm 2018 và phân tích tổng hợp mạng lưới 50 thử nghiệm liên quan đến 12 biện pháp can thiệp tâm lý xã hội khác nhau đối với chứng nghiện amphetamin, methamphetamin, cocaine cho thấy rằng điều trị đa mô thức với cả phương pháp quản lý dự phòng (ontingency management) và phương pháp tiếp cận củng cố cộng đồng và đào tạo gia đình (CRAFT) có hiệu quả cao nhất (tức là tỷ lệ dừng sử dụng chất) và khả năng chấp nhận cao nhất (tức là tỷ lệ tái nghiện thấp nhất).[110] Các phương thức điều trị khác bao gồm đơn trị liệu với quản lý dự phòng hoặc phương pháp tiếp cận củng cố cộng đồng (community reinforcement approach), liệu pháp hành vi nhận thức, chương trình 12 bước,[111] liệu pháp nhóm (non-contingent reward-based therapies), liệu pháp tâm động học (psychodynamic therapy) và các liệu pháp kết hợp khác.[110]
Ngoài ra, nghiên cứu về tác động sinh học thần kinh của tập thể dục cho thấy rằng cái bài tập dùng nhiều oxy (aerobic), đặc biệt là bài tập tập luyện sức bền (ví dụ như chạy marathon), ngăn ngừa sự phát triển của chứng nghiện ma túy và là một liệu pháp bổ trợ hiệu quả cho bệnh nhân nghiện amphetamin. Bệnh nhân tập thể dục có kết quả điều trị tốt hơn, đặc biệt là bệnh nhân nghiện chất kích thích tâm thần.[96][98][112] Đặc biệt, các bài thể dục aerobic làm hạn chế sử dụng tiêm chất kích thích, giảm nguy cơ tái nghiện và làm tăng số lượng thụ thể dopamine D<sub id="mwA3Q">2</sub> (DRD2) trong thể vân[95][112] (do sử dụng chất gây nghiện làm giảm số lượng DRD2 của thể vân).[95] Một nghiên cứu cho thấy rằng tập thể dục cũng có thể ngăn ngừa sự phát triển của hành vi nghiện ma túy bằng cách thay đổi hoạt tính miễn dịch ΔFosB hoặc c-Fos trong thể vân hoặc các vùng khác của hệ thống phần thưởng.[97]Bản mẫu:FOSB addiction table
Sự lệ thuộc vào chất gây nghiện và hội chứng cai
Khả năng dung nạp thuốc tăng lên nhanh chóng khi lạm dụng amphetamin (tức là sử dụng amphetamin để giải trí). Hệ quả, thời gian lạm dụng thuốc kéo dài khiến người nghiện phải tăng liều thuốc ngày càng cao để đạt được tác dụng tương tự.[113][114] Theo một tổng quan hệ thống của tổ chức Cochrane về việc cai nghiện ở những người sử dụng amphetamin và methamphetamin, "khi người dùng liều cao, lâu dài chất gây nghiện bỗng dưng đột ngột ngừng sử dụng amphetamin, hội chứng cai xảy ra trong vòng 24 giờ kể từ liều dùng thuốc cuối cùng. "[115] Tổng quan này lưu ý rằng hội chứng cai ở những người dùng liều cao, dùng lâu dài xảy ra thường xuyên, khoảng 88% trường hợp và kéo dài trong 3–4 tuần.[115] Hội chứng cai amphetamin gồm các triệu chứng: lo lắng, thèm ma túy, khí sắc trầm, mệt mỏi, tăng thèm ăn, tăng hoặc giảm vận động, thiếu động lực, khó ngủ hoặc buồn ngủ, và giấc mơ sáng suốt.[115] Tổng quan hệ thống chỉ ra rằng mức độ nghiêm trọng của các triệu chứng trong hội chứng cai có tương quan thuận với tuổi và mức độ phụ thuộc của từng người.[115] Ngừng điều trị bằng amphetamin ở liều điều trị gây các triệu chứng cai mức độ nhẹ, có thể tránh hội chứng cai bằng cách giảm liều từ từ.[1]
Quá liều
Quá liều amphetamin dẫn đến nhiều triệu chứng khác nhau, nhưng hiếm khi gây tử vong nếu được chăm sóc kịp thời.[1][116] Mức độ nghiêm trọng của các triệu chứng quá liều tăng theo liều lượng và giảm khi có sự dung nạp thuốc với amphetamin.[35] Người nghiện có sự lệ thuộc cơ thể vào thuốc có thể dùng tới 5 gam amphetamin trong một ngày, khoảng 100 lần liều điều trị tối đa hàng ngày. Các triệu chứng của quá liều vừa phải và nặng được liệt kê ở bảng dưới đây. Ngộ độc amphetamin gây tử vong có triệu chứng co giật và hôn mê.[24][35] Năm 2013, sử dụng quá liều amphetamin, methamphetamin và các hợp chất khác có liên quan đến " rối loạn sử dụng amphetamin ", khiến 3788 số ca tử vong trên toàn thế giới (3425–4145 tử vong, khoảng tin cậy 95%). [note 15][117]
| Hệ cơ quan | Quá liều nhẹ hoặc vừa phải[24][35] | Quá liều nặng |
|---|---|---|
| Tim mạch |
| |
| Hệ thần kinh trung ương |
|
|
| Cơ xương khớp |
| |
| Hô hấp |
|
|
| Tiết niệu | ||
| Khác |
|
Độc tính
Ở động vật gặm nhấm và động vật linh trưởng, amphetamin liều đủ cao gây ra độc tính thần kinh dopaminergic, hoặc làm tổn thương neuron dopamine. Tổn thương này đặc trưng bởi sự thoái hóa đuôi sợi trục neuron dopamine và giảm chức năng vận chuyển và thụ thể.[118][119] Không có bằng chứng cho thấy amphetamin gây độc trực tiếp cho thần kinh ở người.[120][121] Tuy nhiên, dùng amphetamin với liều lớn có thể gián tiếp gây ra độc tính thần kinh dopaminergic do tăng thân nhiệt ác tính, hình thành quá mức các loài oxy phản ứng (reactive oxygen species - ROS)[122] và tăng quá trình tự oxy hóa (autoxidation) dopamine. Các mô hình động vật về ngộ độc thần kinh do tiếp xúc với amphetamin liều cao cho thấy sự xuất hiện của tăng thân nhiệt ác tính (tức là nhiệt độ cơ thể ≥ 40 ° C) cần thiết cho quá trình tiến triển ngộ độc thần kinh do amphetamin.[119] Nhiệt độ não tăng trên 40 ° C kéo dài có thể thúc đẩy sự phát triển của độc tính thần kinh do amphetamin ở động vật thí nghiệm bằng cách tạo ra các loại oxy phản ứng, phá vỡ chức năng protein tế bào và tăng tính thấm của hàng rào máu não.[119]
Rối loạn tâm thần
Quá liều amphetamin có thể dẫn đến rối loạn tâm thần do sử dụng chất. Các triệu chứng: hoang tưởng và rối loạn hoang tưởng paranoid.[123][37] Một tổng quan hệ thống của tổ chức Cochrane về điều trị rối loạn tâm thần bằng amphetamin, dextroamphetamin và methamphetamin cho thấy khoảng 5–15% người nghiện không thể khỏi hoàn toàn.[124] Theo tổng quan, có ít nhất một thử nghiệm cho thấy thuốc chống loạn thần giải quyết hiệu quả các triệu chứng của rối loạn tâm thần do sử dụng amphetamin cấp tính. Rối loạn tâm thần hiếm khi phát sinh từ việc sử dụng các liệu pháp chữa trị.[24][37][38]
Tương tác thuốc
Nhiều loại dược chất được biết là có tương tác với amphetamin, dẫn đến tác dụng và/hoặc chuyển hóa của thuốc bị thay đổi.[24] Chất ức chế enzym chuyển hóa amphetamin (ví dụ, CYP2D6 và FMO3) kéo dài thời gian bán thải của amphetamin, có nghĩa là tác dụng của chất sẽ kéo dài hơn.[24] Amphetamin cũng tương tác với MAOIs, đặc biệt là chất ức chế monoamine oxidase A, vì cả MAOI và amphetamin đều làm tăng catecholamine trong huyết tương (tức là noradrenalin và dopamine);[24] do đó, việc sử dụng đồng thời cả hai chất rất nguy hiểm.[24] Amphetamin làm thay đổi tác dụng của hầu hết các loại thuốc thần kinh. Đặc biệt, amphetamin có thể làm giảm tác dụng của thuốc an thần và thuốc ức chế thần kinh, đồng thời làm tăng tác dụng của thuốc kích thần và thuốc chống trầm cảm.[24] Amphetamin cũng có thể làm giảm tác dụng của thuốc hạ huyết áp và thuốc chống loạn thần do tác dụng của chất lên huyết áp và dopamine.[24] Bổ sung kẽm có thể làm giảm liều có hiệu quả tối thiểu (ED) của amphetamin trong điều trị ADHD.[125]
Không có tương tác đáng kể khi dùng amphetamin với thức ăn, nhưng độ pH của đường tiêu hóa và nước tiểu ảnh hưởng đến sự hấp thu và bài tiết của amphetamin, tương ứng.[24] Các chất có tính acid làm giảm hấp thu amphetamin và tăng bài tiết qua nước tiểu, còn các chất có tính kiềm thì ngược lại.[24] Do ảnh hưởng của pH đối với sự hấp thụ, amphetamin cũng tương tác với thuốc làm giảm độ acid dịch vị dạ dày như thuốc ức chế bơm proton và thuốc kháng histamine H2, làm tăng pH đường tiêu hóa (tức là kiềm hơn).[24]
Dược học
Dược lực học

Amphetamin phát huy tác dụng bằng cách sử dụng chất dẫn truyền thần kinh monoamin làm tín hiệu thần kinh trong não, chủ yếu ở tế bào thần kinh catecholamin trong con đường điều hành chức năng (executive function pathway) và và con đường khen thưởng (reward pathway) của não.[33][51] Nồng độ của các chất dẫn truyền thần kinh (dopamine và noradrenalin) có liên quan đến con đường điều hành chức năng và phần thưởng dopamine và noradrenalin. Nồng độ các chất này tăng đột ngột, phụ thuộc vào liều lượng của amphetamin vì tác dụng của amphetamin đối với các chất vận chuyển monoamin.[33][51][126] Các tác dụng tăng cường và thúc đẩy động lực của amphetamin chủ yếu là do tăng cường hoạt động dopaminergic trong con đường trung não-hồi viền.[22] Tác dụng hưng phấn và kích thích vận động của amphetamin phụ thuộc vào cường độ và tốc độ bằng cách tăng nồng độ dopamine và noradrenalin ở synap trong thể vân.[2]
Năm 2001, amphetamin được chứng minh chất chủ vận mạnh của trace amine-associated receptor 1 (TAAR1), một thụ thể bắt cặp với protein G (GPCR) ở đây là protein Gs và Gq. Phát hiện này rất quan trọng trong việc điều hòa các monoamine trong não..[33][132] Kích hoạt TAAR1 làm tăng sản xuất cAMP thông qua hoạt hóa adenylyl cyclase và ức chế chức năng vận chuyển monoamin.[33][133] Các autoreceptor monoamine (ví dụ, receptor dopamin D2, receptor α2-adrenergic, và receptor 5-HT1) có tác dụng ngược lại với TAAR1, và khi các receptor (thụ thể) này phối hợp phối hợp với nhau sẽ điều hòa cho quá trình vận chuyển các monoamine.[33][34] Đặc biệt, amphetamin và các trace amin có ái lực liên kết cao đối với TAAR1, nhưng không có ái lực liên kết đối với các autoreceptor monoamine.[33][34] Các nghiên cứu hình ảnh học chỉ ra rằng amphetamin và trace amin ức chế quá trình tái hấp thu monoamine tùy vị trí đặc trưng và phụ thuộc vào có hay không sự có mặt của TAAR1 trong các tế bào thần kinh monoamin.[33]
Ngoài việc ức chế các protein vận chuyển monoamin, amphetamin còn ức chế cả chất vận chuyển monoamine trong túi synap gồm VMAT1, VMAT2, SLC1A1, SLC22A3 và SLC22A5. SLC1A1 là chất vận chuyển amino acid kích thích 3 (Excitatory amino acid transporter 3, EAAT3), một chất vận chuyển glutamat nằm trong tế bào thần kinh. SLC22A3 là chất vận chuyển monoamine ngoài thần kinh có trong tế bào thần kinh đệm hình hình sao. SLC22A5 là chất vận chuyển carnitine có ái lực cao. Amphetamin làm tăng biểu hiện gen phiên mã điều hòa cocain và amphetamin (cocaine- and amphetamin-regulated transcript, CART).[134] CART là neuropeptide liên quan đến hành vi ăn uống, căng thẳng và hành vi khen thưởng, gây ra sự gia tăng quá trình phát triển và tồn tại của các tế bào thần kinh trong ống nghiệm.[9][135][136] Thụ thể CART vẫn chưa được xác định, nhưng có bằng chứng đáng kể cho thấy CART chỉ liên kết với thụ thể bắt cặp với protein G (GPCR) ở đây là protein Gi và Go.[136][137] Amphetamin cũng ức chế monoamine oxidase ở liều rất cao, dẫn đến chuyển hóa monoamine và amine trace ít hơn. Hậu quả, nồng độ monoamine synap tăng.[138][139] Ở người, thụ thể hiện tại được biết duy nhất ở màng sau synap mà amphetamin gắn được là thụ thể 5-HT1A.[140][141]
Tác dụng ngắn hạn của amphetamin ở người là do tăng cường dẫn truyền thần kinh, dưới tác dụng của dopamine,[33] serotonin,[33] noradrenalin,[33] adrenalin,[126] histamine,[126] CART peptide,[134] opioid nội sinh,[142][143][144] hormone vỏ thượng thận,[145][146] corticosteroid,[145][146] và glutamate, thông qua tương tác với CART, 5-HT1A, EAAT3, TAAR1, VMAT1, VMAT2 và các mục tiêu sinh học khác. Amphetamin cũng kích hoạt 7 enzym carbonic anhydrase, một trong 7 enzym này có mặt trong não người.
Dextroamphetamin là một chất chủ vận mạnh của TAAR1 hơn levoamphetamin.[147] Do đó, dextroamphetamin tạo ra kích thích lên hệ TKTW lớn hơn levoamphetamin, gần gấp 3 đến 4 lần, nhưng levoamphetamin có tác dụng lên hệ tim mạch và tác dụng ngoại vi mạnh hơn.[35][147]
Dopamine
Ở một số vùng não nhất định, amphetamin làm tăng nồng độ dopamine trong khe synap.[33] Amphetamin có thể xâm nhập vào tế bào thần kinh trước synap thông qua chất vận chuyển dopamine (DAT) hoặc bằng cách khuếch tán trực tiếp qua màng tế bào thần kinh.[33] Amphetamin ức chế tái hấp thu cạnh tranh ở chất vận chuyển dopamine.[33] Khi đi vào tế bào thần kinh trước synap, amphetamin sẽ kích hoạt TAAR1 thông qua tín hiệu protein kinase A (PKA) và protein kinase C (PKC), gây ra quá trình phosphoryl hóa DAT.[33] Quá trình phosphoryl hóa nhờ PKC và PKA này dẫn đến nhập bào DAT (ức chế tái hấp thu không cạnh tranh), nhưng riêng sự phosphoryl hóa nhờ PKC gây ra sự vận chuyển ngược dopamine (tức là dopamine chui ra ngoài tế bào).[33][148] Amphetamin làm tăng nồng độ calci nội bào. Tác dụng này có liên quan đến quá trình phosphoryl hóa DAT thông qua con đường Ca2+/calmodulin-dependent protein kinase (CAMK), làm thất thoát dopamin ra ngoài.[132][131] Thông qua việc kích hoạt trực tiếp các kênh kali điều chỉnh bên trong bắt cặp với protein G (G protein-coupled inwardly-rectifying potassium channel, GIRK), TAAR1 làm giảm tốc độ kích hoạt tế bào thần kinh dopamine, ngăn ngừa trạng thái cường dopaminergic.[128][129][149]
Amphetamin cũng là chất nền cho chất vận chuyển monoamine dạng túi synap, VMAT2.[126][127] Sau khi hấp thu amphetamin tại VMAT2, amphetamin làm vỡ các túi synap ở khe synap, giải phóng các phân tử dopamine từ các túi synap vào tế bào nhờ dòng chảy dopamine qua VMAT2.[126][127] Sau đó, các phân tử dopamine trong tế bào được giải phóng từ tế bào thần kinh trước synap vào khe synap thông qua sự vận chuyển thông qua chất vận chuyển dopamine (DAT) theo chiều ngược lại.[33][126][127]
Noradrenalin (norepinephrin)
Tương tự như dopamine, liều amphetamin tùy thuộc vào mức độ của noradrenalin, tiền chất của adrenalin.[51] Dựa trên biểu hiện mRNA của TAAR1 trong neuron, amphetamin được cho là có tác động đến noradrenalin tương tự như dopamine.[33][126][148] Nói cách khác, amphetamin gây ra thất thoát noradrenalin nhờ TAAR1 và ức chế tái hấp thu không cạnh tranh tại chất vận chuyển noradrenalin được được phosphoryl hóa (phosphorylated norepinephrine transporter, phosphorylated NET), ức chế tái hấp thu cạnh tranh tại chất vận chuyển noradrenalin (norepinephrine transporter, NET) và giải phóng noradrenalin từ chất vận chuyển monoamine dạng túi synap VMAT2.[33][126]
Serotonin
Amphetamin có tác dụng tương tự trên serotonin như trên dopamine và norepinephrine (nhưng ít rõ rệt hơn).[33][51] Amphetamin ảnh hưởng đến serotonin thông qua chất vận chuyển monoamine dạng túi synap VMAT2. Giống cơ chế của noradrenalin, amphetamin làm thất thoát serotonin nhờ TAAR1 và ức chế tái hấp thu không cạnh tranh tại chất vận chuyển serotonin được được phosphoryl hóa (phosphorylated serotonin transporter, phosphorylated SERT).[33][126] Giống như dopamine, amphetamin có ái lực thấp với thụ thể 5-HT1A của người.[140][141]
Các chất dẫn truyền thần kinh, peptide, hormon và enzym khác
Sử dụng amphetamin cấp tính ở người làm tăng giải phóng opioid nội sinh trong một số cấu trúc não thuộc hệ thống phần thưởng.[142][143][144] Khi tiếp xúc với amphetamin, nồng độ glutamat ngoại bào và nồng độ chất dẫn truyền thần kinh trong não được chứng minh là tăng trong thể vân. Sự gia tăng nồng độ glutamat ngoại bào này có lẽ xảy ra thông qua cơ chế liên quan đến EAAT3 (một chất vận chuyển tái hấp thu glutamate) trong tế bào thần kinh dopamine. Amphetamin cũng gây ra sự giải phóng chọn lọc histamin từ các tế bào mast và làm thoát histamin từ các tế bào thần kinh histaminergic thông qua VMAT2.[126] Sử dụng amphetamin làm tăng nồng độ hormone vỏ thượng thận và corticosteroid trong huyết tương bằng cách kích thích trục hạ đồi-tuyến yên-tuyến thượng thận.[31][145][146]
Tháng 12 năm 2017, nghiên cứu đầu tiên đánh giá sự tương tác giữa amphetamin và enzym carbonic anhydrase ở người đã được công bố; trong số 11 enzym carbonic anhydrase được đưa vào nghiên cứu, amphetamin kích hoạt mạnh mẽ 7 enzym, trong đó có 4 enzym có mặt trong não người. Dựa trên nghiên cứu tiền lâm sàng, kích hoạt enzym carbonic anhydrase trong não có tác dụng nâng cao nhận thức.[150] Tuy nhiên, dựa trên việc sử dụng lâm sàng các chất ức chế carbonic anhydrase, sự hoạt hóa carbonic anhydrase trong các mô khác có thể gây ra tác dụng phụ, chẳng hạn như làm trầm trọng thêm bệnh glôcôm.[150]
Dược động học
Sinh khả dụng đường uống của amphetamine thay đổi theo pH đường tiêu hóa.[24] Amphetamine được hấp thụ tốt ở ruột và sinh khả dụng thường trên 75% đối với dextroamphetamine. Amphetamine là một base yếu với pKa là 9,9. Do đó, khi môi trường có pH kiềm, phần lớn hoạt chất nằm ở dạng base tự do hòa tan trong lipid, và được hấp thu qua màng tế bào giàu lipid của biểu mô ruột.[24] Ngược lại, khi môi trường có pH toan, có nghĩa là hoạt chất chủ yếu ở dạng cation (muối) hòa tan trong nước và ít được hấp thu hơn. Khoảng 20% amphetamine đi trong hệ tuần toàn được liên kết với protein huyết tương. Sau khi hấp thụ, amphetamine dễ dàng phân phối vào hầu hết các mô trong cơ thể. Amphetamine có nồng độ cao tại dịch não tủy và mô não.[15]The half-lives of amphetamine enantiomers differ and vary with urine pH.[3] At normal urine pH, the half-lives of dextroamphetamine and levoamphetamine are 9–11 hours and 11–14 hours, respectively.[3] Highly acidic urine will reduce the enantiomer half-lives to 7 hours;[15] highly alkaline urine will increase the half-lives up to 34 hours.[15] The immediate-release and extended release variants of salts of both isomers reach peak plasma concentrations at 3 hours and 7 hours post-dose respectively.[3] Amphetamine is eliminated via the kidneys, with 30–40% of the drug being excreted unchanged at normal urinary pH.[3] When the urinary pH is basic, amphetamine is in its free base form, so less is excreted.[3] When urine pH is abnormal, the urinary recovery of amphetamine may range from a low of 1% to a high of 75%, depending mostly upon whether urine is too basic or acidic, respectively.[3] Following oral administration, amphetamine appears in urine within 3 hours.[15] Roughly 90% of ingested amphetamine is eliminated 3 days after the last oral dose.[15]
Lisdexamfetamine is a prodrug of dextroamphetamine.[151][152] It is not as sensitive to pH as amphetamine when being absorbed in the gastrointestinal tract.[152] Following absorption into the blood stream, lisdexamfetamine is completely converted by red blood cells to dextroamphetamine and the amino acid L-lysine by hydrolysis via undetermined aminopeptidase enzymes.[152][151][153] This is the rate-limiting step in the bioactivation of lisdexamfetamine.[151] The elimination half-life of lisdexamfetamine is generally less than 1 hour.[152][151] Due to the necessary conversion of lisdexamfetamine into dextroamphetamine, levels of dextroamphetamine with lisdexamfetamine peak about one hour later than with an equivalent dose of immediate-release dextroamphetamine.[151][153] Presumably due to its rate-limited activation by red blood cells, intravenous administration of lisdexamfetamine shows greatly delayed time to peak and reduced peak levels compared to intravenous administration of an equivalent dose of dextroamphetamine.[151] The pharmacokinetics of lisdexamfetamine are similar regardless of whether it is administered orally, intranasally, or intravenously.[151][153] Hence, in contrast to dextroamphetamine, parenteral use does not enhance the subjective effects of lisdexamfetamine.[151][153] Because of its behavior as a prodrug and its pharmacokinetic differences, lisdexamfetamine has a longer duration of therapeutic effect than immediate-release dextroamphetamine and shows reduced misuse potential.[151][153]
Cho đến hiện tịa, CYP2D6, dopamine β-hydroxylase (DBH), monooxygenase chứa flavin 3 (flavin-containing monooxygenase 3, FMO3), butyrate-CoA ligase (XM-ligase), và glycine N-acyltransferase (GLYAT) là các enzym được biết đến có tham gia chuyển hóa amphetamin hoặc các chất trung gian ở người. Amphetamin có nhiều loại sản phẩm chuyển hóa gồm 4-hydroxyamphetamine, 4-hydroxynorephedrine, 4-hydroxyphenylacetone, acid benzoic, acid hippuric, norephedrine và phenylaceton. Trong số các chất chuyển hóa này, chất kích thích giao cảm có hoạt tính là 4-hydroxyamphetamine,[154] 4-hydroxynorephedrine,[155] và norephedrine.[156] Các con đường chuyển hóa chính liên quan đến quá trình para-hydroxyl hóa nhân thơm, alpha- và betahydroxyl hóa hợp chất không vòng, N-oxy hóa, N-dealkyl hóa, và khử amin.[157] Các con đường trao đổi chất, các chất trung gian chuyển hóa đã được phát hiện và các enzym chuyển hóa ở người được trình bày trong sơ đồ dưới đây:
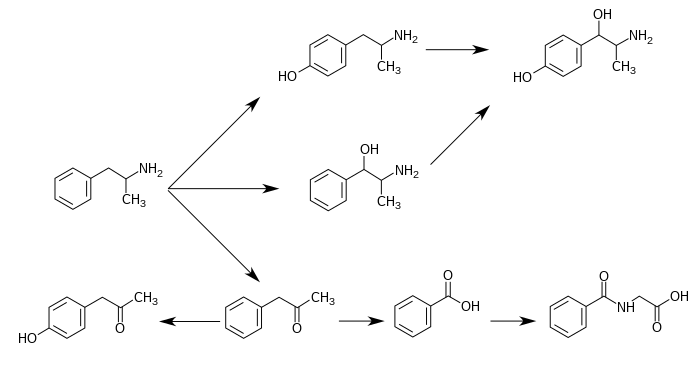
Dược-vi sinh-di truyền học (Pharmacomicrobiomic)
Metagenome của người (tức là các vật liệu di truyền của một cá thể và các vật liệu di truyền của tất cả các vi sinh vật có mặt trên hoặc bên trong cơ thể của cá thể đó) rõ ràng là rất khác nhau giữa các cá thể.[163][164] Vì tổng số tế bào vi sinh vật và virus trong cơ thể người (hơn 100 nghìn tỷ) nhiều hơn rất nhiều tế bào người (hàng chục nghìn tỷ),[163][165] nên có khả năng tương tác đáng kể giữa thuốc và hệ vi sinh vật của một cá thể. Những tương tác đó bao gồm:[163][164][166]
- thuốc làm thay đổi thành phần của hệ vi sinh vật ở người,
- vi sinh vật tiết các enzym làm thay đổi dược động học của thuốc
- sự chuyển hóa thuốc của vi sinh vật ảnh hưởng đến hiệu quả lâm sàng và độc tính của thuốc.
Lĩnh vực nghiên cứu những tương tác này được gọi là Dược-vi sinh-di truyền học (Pharmacomicrobiomic).[163]
Tương tự như hầu hết các phân tử sinh học và chất lạ sinh học (xenobiotic)[167] dùng đường uống, amphetamin sẽ phải trải qua quá trình chuyển hóa mạnh mẽ bởi hệ vi khuẩn chí đường ruột của con người trước khi hấp thụ vào máu.[166] Enzyme vi sinh vật chuyển hóa amphetamin đầu tiên là tyramine oxidase do một chủng vi khuẩn E. coli tiết ra đã được xác định vào năm 2019.[166] Enzyme chuyển hóa amphetamin, tyramin và phenethylamine với ái lực liên kết gần giống nhau đối với cả ba hợp chất.[166]
Các hợp chất nội sinh liên quan
Amphetamin có cấu trúc và chức năng rất giống với các trace amin nội sinh, là các phân tử điều hòa thần kinh tự nhiên được tạo ra trong cơ thể và não người.[33][168] Trong nhóm này, các hợp chất có liên quan chặt chẽ nhất là phenethylamin (hợp chất gốc của amphetamin) và N-methylphenethylamine (một đồng phân của amphetamin, tức là N-methylphenethylamine và amphetamin có công thức phân tử giống hệt nhau).[33][169] Ở người, phenethylamine được sản xuất trực tiếp từ L-phenylalanine nhờ enzyme aromatic L-amino acid decarboxylase (AADC), enzyme này cũng chuyển L-DOPA thành dopamine.[169] Đổi lại, N-methylphenethylamine được chuyển hóa từ phenethylamine nhờ enzyme phenylethanolamine N -methyltransferase (cùng một loại enzyme chuyển hóa noreadrenalin thành adrenalin).[169] Giống như amphetamin, cả phenethylamine và N-methylphenethylamine có chức năng điều hòa dẫn truyền thần kinh monoamine thông qua TAAR1.[33][168][169] Tuy nhiên, không giống như amphetamin, cả hai chất này đều bị phân hủy bởi monoamine oxidase B, và do đó có thời gian bán hủy ngắn hơn amphetamin.[169]
Hoá học
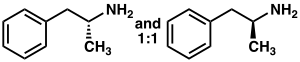


Phenyl-2-nitropropene (right cups)
Amphetamin là một chất thuộc dãy đồng đẳng của chất dẫn truyền thần kinh phenethylamine động vật có vú. Công thức hóa học là C
9H
13N. Nguyên tử carbon gắn nhóm chức amin là trung tâm lập thể và amphetamin được cấu tạo từ hỗn hợp racemic của hai chất đối quang (enantiomer) với tỷ lệ 1:1. Hỗn hợp racemic này có thể phân tách thành các đồng phân quang học là levoamphetamin và dextroamphetamin.[9] Ở nhiệt độ phòng, dạng base tự do của amphetamin là chất lỏng, không màu và dễ bay hơi với mùi amin đặc trưng, vị chát.[19] Amphetamin dạng muối ở thể rắn, gồm amphetamin adipat,[170] aspartat,[24] hydrochloride,[171] phosphat,[172] saccharat,[24] sulfat,[24] và tannat.[173] Dextroamphetamin sulfat là muối enantiopure (có sẵn ở một dạng lập thể cụ thể) phổ biến nhất. Amphetamin cũng là hợp chất gốc của lớp amphetamin thay thế, gồm một số dẫn xuất có tác dụng lên thần kinh.[9] Trong hóa học hữu cơ, amphetamin là một phối tử chiral (chiral ligand) rất hữu ích trong tổng hợp chọn lọc lập thể chất 1,1'-bi-2-naphthol.[174]
Các dẫn xuất
Các dẫn xuất của amphetamin, hoặc "amphetamin thay thế", là các hợp chất sử dụng cấu trúc hóa học của amphetamin như một "xương sống".[175][176] Nói một cách dễ hiểu, thay thế một hoặc nhiều nguyên tử hydro trong cấu trúc amphetamin bằng các nhóm thế sẽ tạo ra các dẫn xuất.[177] Các dẫn xuất amphetamin gồm các chất kích thần như methamphetamin, các chất kích thần và gây ảo giác qua cơ chế serotonergic như MDMA (thuốc lắc) và thuốc thông mũi như ephedrin, v.v....[175][176]
Tổng hợp
Năm 1887 ghi nhận quy trình đầu tiên tổng hợp amphetamin.[178] từ thời điểm đó trở đi, ngày càng có nhiều con đường tổng hợp amphetamin.[179][180] Con đường phổ biến nhất của tổng hợp amphetamin hợp pháp và bất hợp pháp là sử dụng quá trình khử phi kim được gọi là phản ứng Leuckart (phương pháp 1).[181] Trong bước đầu tiên, phenylacetone phản ứng với formamide, có thể bổ sung acid formic, để tạo ra N-formylamphetamine. Chất trung gian này sau đó được thủy phân bằng cách sử dụng acid hydrochloric, và sau đó base hóa, chiết xuất bằng dung môi hữu cơ, ngưng tụ và chưng cất để tạo ra dạng base tự do. Base tự do sau đó được hòa tan trong dung môi hữu cơ, thêm acid sulfuric, cho ra thành phẩm amphetamin kết tủa dưới dạng muối sulfat.[181][182]
Một số phương pháp phân giải chiral (chiral resolution) được phát triển để tách hai đồng phân quang học của amphetamin.[179] Ví dụ, hỗn hợp racemic amphetamin có thể được xử lý bằng d-tartaric acid để tạo thành một muối của đồng phân không đối quang (diastereomer), sau đó kết tinh phân đoạn để tạo ra dextroamphetamin. Phân giải chiral vẫn là phương pháp kinh tế nhất để thu được amphetamin tinh khiết về mặt quang học trên quy mô lớn.[183] Ngoài ra, một số quy trình tổng hợp chọn lọc lập thể của amphetamin đã được phát triển. Ví dụ, (R)-1-phenyl-ethanamine tinh khiết về mặt quang học được cô đặc với phenylacetone để tạo ra base Schiff chiral. Trong bước tổng hợp then chốt, chất trung gian này được khử bằng cách hydro hóa, thay đổi tính đối xứng của nguyên tử carbon alpha bằng nhóm amin. Phân cắt liên kết amin benzylic bằng phản ứng hydro hóa tạo ra dextroamphetamin tinh khiết về mặt quang học.[183]
Một số lượng lớn các con đường tổng hợp thay thế cho amphetamin đã được phát triển dựa trên các phản ứng hữu cơ cổ điển.[179][180]
- Phản ứng Friedel – Crafts alkyl hóa benzen bằng allyl chloride để tạo ra beta chloropropylbenzen, sau đó phản ứng với amoniac để tạo ra racemic amphetamin (phương pháp 2).[184]
- Phản ứng Ritter (phương pháp 3). Trong con đường này, allylbenzen phản ứng với acetonitril trong acid sulfuric để tạo ra organosulfat, sau đó cho phản ứng tiếp với natri hydroxide để tạo ra amphetamin thông qua chất trung gian acetamide.[185][186]
- Alkyl hóa hợp chất ethyl 3-oxobutanoat (còn gọi là ethyl acetoacetat) bằng methyl iodide, tiếp theo cho sản phẩm thu được phản ứng với benzyl chloride để chuyển thành acid 2-methyl-3-phenyl-propanoic. Chất trung gian này chuyển vị thành amphetamin bằng cách sử dụng chuyển vị Hofmann hoặc chuyển vị Curtius (phương pháp 4).
Một số lượng đáng kể amphetamin được tổng hợp bằng cách khử nhóm nitro, imine, oxime, hoặc các nhóm chức chứa nitơ khác.[180]
- Ngưng tụ Knoevenagel giữa benzaldehyde với nitroethan tạo ra phenyl-2-nitropropen. Liên kết đôi và nhóm nitro của chất trung gian này bị khử bằng cách hydro hóa có xúc tác hoặc khử bằng lithi nhôm hydride (LiAlH4) (phương pháp 5).[181][187]
- Một phương pháp khác là phản ứng của phenylaceton với amonia, tạo ra chất trung gian imine, sau đó sử dụng hydro có xúc tác paladi hoặc lithi nhôm hydride (LiAlH4) khử sản phẩm trên thành amin bậc một (phương pháp 6).[181]
Phát hiện trong dịch cơ thể
Trong thể thao, công việc, hay để chẩn đoán ngộ độc và công tác giám định pháp y không thể thiếu các xét nghiệm phát hiện amphetamin trong nước tiểu hoặc máu. Xét nghiệm miễn dịch là hình thức xét nghiệm amphetamin phổ biến nhất, tuy nhiên có thể phản ứng chéo với một số loại thuốc cường giao cảm.[188] Phương pháp sắc ký dành riêng cho amphetamin giúp hạn chế các kết quả dương tính giả.[189] Kỹ thuật tách chiral giúp phân biệt nguồn gốc của thuốc, liệu là amphetamin kê đơn, amphetamin dạng tiền chất kê đơn, (ví dụ: selegiline), sản phẩm thuốc không kê đơn có chứa levomethamphetamin, [note 20] hay amphetamin thay thế do sản xuất bất hợp pháp.[189][190][191] Một số loại thuốc kê đơn sản xuất amphetamin dưới dạng chất chuyển hóa, bao gồm benzphetamin, clobenzorex, famprofazone, fenproporex, lisdexamfetamin, mesocarb, methamphetamin, prenylamine và selegiline,v...v.[2][192][193] Xét nghiệm ma túy đối với những người sử dụng những dược chất trên có thể cho kết quả dương tính với amphetamin.[192][193] Amphetamin thường chỉ phát hiện được bằng xét nghiệm ma túy trong khoảng 24 giờ, mặc dù nếu dùng liều cao thì vẫn có thể phát hiện trong 2–4 ngày kể từ liều cuối cùng.[188]
Đối với các xét nghiệm, có nghiên cứu lưu ý rằng kỹ thuật xét nghiệm miễn dịch nhân lên bằng enzym (Enzyme multiplied immunoassay technique, EMIT) đối với amphetamin và methamphetamin có nhiều kết quả dương tính giả hơn so với phương pháp sắc ký lỏng-khối phổ (LC-MS).[190] Sắc ký khí-khối phổ (GC–MS)amphetamin và methamphetamin với thuốc thử dẫn xuất (S)-(−)-trifluoroacetylprolyl chloride cho phép phát hiện methamphetamin trong nước tiểu.[189] GC–MS amphetamin và methamphetamin với thuốc thử chiral là acid Mosher cho phép phát hiện cả dextroamphetamin và dextromethamphetamin trong nước tiểu.[189] Do đó, phương pháp này được sử dụng trên các mẫu có kết quả dương tính, giúp phân biệt nguồn gốc của thuốc.[189]
Lịch sử, xã hội và văn hóa
| Chất gây nghiện | Ước tính | Thấp nhất | Cao nhất |
|---|---|---|---|
| Amphetamin (và các chất tương tự) | 34 | 29 | 41 |
| Cần sa | 209 | 149 | 265 |
| Cocain | 21 | 18 | 26 |
| Thuốc lắc (hay ecstasy, MDMA) | 20 | 9 | 36 |
| Opioid | 61 | 37 | 78 |
Chất kích thích dạng amphetamin ban đầu có nguồn gốc từ cây Ma hoàng, có chứa ephedrin, được người Trung Quốc sử dụng khoảng 5.000 trước.[196][197] Ephedrin được phân lập từ Ephedra vulgaris ở Nhật Bản vào năm 1885 và được nghiên cứu các đặc tính y học của cây trong suốt thập niên 1920.[196] Do hàm lượng ephedrin trong cây Ephedra quá ít nên đã thúc đẩy việc tìm kiếm chất tương tựephedrin.[196]
Amphetamin được tổng hợp lần đầu tiên vào năm 1887 tại Đức, do nhà hóa học người Romania Lazăr Edeleanu. Ông đặt tên cho chất là phenylisopropylamine;[178][198][199] 40 năm sau, vào năm 1927, đặc tính kích thích của loại thuốc này được khám phá. Gordon Alles tái tổng hợp chất và cho rằng chất này có đặc tính kích thích giao cảm.[199] Cuối năm 1933, Smith, Kline và French bắt đầu bán dưới dạng thuốc hít, tên thương mại là Benzedrine, để làm thuốc thông mũi.[25] 3 năm sau, benzedrine sulfat được đưa vào sử dụng để điều trị nhiều loại bệnh lý khác nhau, bao gồm chứng ngủ rũ, béo phì, huyết áp thấp, giảm ham muốn (ICD-10: F52.0) và đau mạn tính, v.v...[42][25] Trong Chiến tranh thế giới thứ hai, amphetamin và methamphetamin được sử dụng rộng rãi bởi cả phe Đồng minh và phe Trục vì tác dụng kích thích và nâng cao độ tỉnh táo, nhuệ khí cho binh lính.[178][200][201] Chính phủ các nước bắt đầu kiểm soát chặt chẽ việc bán amphetamin khi phát hiện các đặc tính gây nghiện của ma túy.[178] Đầu những năm 1970 ở Hoa Kỳ, amphetamin được xếp vào danh sách chất phải kiểm soát theo Đạo luật Kiểm soát Chất.[202][203] Bất chấp sự kiểm soát nghiêm ngặt của chính phủ, amphetamin vẫn được nhiều người thuộc đa ngành nghề, đa lĩnh vựng sử dụng hợp pháp hoặc bất hợp pháp, bao gồm các nhà văn,[204] nhạc sĩ,[205] nhà toán học,[206] và vận động viên.
Amphetamin ngày nay vẫn được tổng hợp bất hợp pháp trong các phòng thí nghiệm bí mật và được bán trên thị trường chợ đen, chủ yếu ở các nước châu Âu.[207] Tính đến năm 2018[cập nhật], trong các quốc gia thành viên của Liên minh Châu Âu (EU), có 11,9 triệu người trưởng thành trong độ tuổi 15–64 đã sử dụng amphetamin hoặc methamphetamin ít nhất một lần trong đời và 1,7 hàng triệu người đã sử dụng trong năm 2017.[208] Trong năm 2012, khoảng 5,9 tấn amphetamin bất hợp pháp đã bị thu giữ trong các nước thành viên EU.[209] "Giá bán trên đường phố" amphetamin bất hợp pháp trong EU dao động từ 6–38 € mỗi gam (khoảng 170.000 đến 1.070.000 đồng, theo tỷ giá EUR-VND năm 2014).[209] Bên ngoài châu Âu, thị trường chợ đen chất amphetamin nhỏ hơn nhiều so với thị trường methamphetamin và MDMA.[207]
Tình trạng pháp lý
Theo kết quả của Công ước Liên hợp quốc năm 1971 về các chất hướng thần, amphetamin đã trở thành chất bị kiểm soát ở tất cả 183 quốc gia thành viên.[26] Do đó, amphetamin được quản lý chặt chẽ ở hầu hết các quốc gia.[210][211] Một số quốc gia, chẳng hạn như Hàn Quốc và Nhật Bản, đã cấm amphetamin thay thế ngay cả khi sử dụng chất trong y tế.[212][213] Ở các quốc gia khác, chẳng hạn như Canada,[214] Hà Lan,[215] Hoa Kỳ,[24] Úc,[216] Thái Lan,[217] và Vương quốc Anh,[218] amphetamin nằm trong mục thuốc bị kiểm soát trong dược thư quốc gia, vẫn được cho phép sử dụng để điều trị y tế.[207]
Dược phẩm
Một số công thức amphetamin được bán trên thị trường hiện có chứa cả hai đối quang, gồm Adderall, Adderall XR, Mydayis, Adzenys ER, Adzenys XR-ODT, Dyanavel XR, Evekeo và Evekeo ODT. Trong đó, Evekeo (bao gồm Evekeo ODT) là sản phẩm duy nhất chỉ chứa racemic amphetamin (như amphetamin sulfat), và do đó đây là sản phẩm duy nhất có nhóm chức hoạt động của "amphetamin".[1][31] Dextroamphetamin, được bán trên thị trường dưới tên thương hiệu Dexedrine và Zenzedi, là sản phẩm amphetamin dạng enantiopure (đối quang tinh khiết) duy nhất hiện có. Một dạng tiền chất của dextroamphetamin là lisdexamfetamin được bày bán trên thị trường dưới tên thương hiệu Vyvanse. Vì là một tiền chất, lisdexamfetamin có cấu trúc khác với dextroamphetamin và không hoạt động cho đến khi thuốc được chuyển hóa thành dextroamphetamin.[152] Racemic amphetamin trước đây mang tên thương mại là Benzedrine, Psychedrine và Sympatedrine.[2] Levoamphetamin trước đây có tên thương mại là Cydril.[2] Nhiều dược phẩm amphetamin hiện tại là muối do khi ở dạng base tự do, thuốc có tính bay hơi tương đối cao.[2] Tuy nhiên, dạng bào chế hỗn dịch uống và viên nén rã (ODT) chứa dạng base tư do của thuốc được giới thiệu năm 2015 và 2016.[219][220] Sau đây là một số tên thương mại của thuốc và thành phần của chúng.
| Tên thương mại | Hoạt chất | Tỷ lệ đối quang | Bào chế | Năm bắt đầu sản xuất | Dữ liệu tại Hoa Kỳ | Nguồn |
|---|---|---|---|---|---|---|
| Adderall | - | 3: 1 (muối) | viên nén | 1996 | GoodRx | [2] |
| Adderall XR | - | 3: 1 (muối) | viên con nhộng | 2001 | GoodRx | [2] |
| Mydayis | - | 3: 1 (muối) | viên con nhộng | 2017 | GoodRx | [221][222] |
| Adzenys ER | amphetamin | 3: 1 (base) | hỗn dịch uống | 2017 | GoodRx | [223] |
| Adzenys XR-ODT | amphetamin | 3: 1 (base) | viên nén rã | 2016 | GoodRx | [220][224] |
| Dyanavel XR | amphetamin | 3,2: 1 (base) | hỗn dịch uống | 2015 | GoodRx | [219] |
| Evekeo | amphetamin sulfat | 1: 1 (muối) | viên nén | 2012 | GoodRx | [31][225] |
| Evekeo ODT | amphetamin sulfat | 1: 1 (muối) | viên nén rã | 2019 | GoodRx | [226] |
| Dexedrine | dextroamphetamin sulfat | 1: 0 (muối) | viên con nhộng | Năm 1976 | GoodRx | [2] |
| Zenzedi | dextroamphetamin sulfat | 1: 0 (muối) | viên nén | 2013 | GoodRx | [227] |
| Vyvanse | lisdexamfetamin dimesylate | 1: 0 (tiền chất) | viên con nhộng | 2007 | GoodRx | [2][152][228] |
| viên nén | ||||||
| Xelstrym | dextroamphetamin | 1: 0 (base) | thuốc dán | 2022 | GoodRx | [229] |
- ^ a b c d e f g h i Stahl SM (tháng 3 năm 2017). “Amphetamine (D,L)”. Prescriber's Guide: Stahl's Essential Psychopharmacology (ấn bản 6). Cambridge, United Kingdom: Cambridge University Press. tr. 45–51. ISBN 9781108228749. Truy cập ngày 5 tháng 8 năm 2017.
- ^ a b c d e f g h i j k l Heal DJ, Smith SL, Gosden J, Nutt DJ (tháng 6 năm 2013). “Amphetamine, past and present – a pharmacological and clinical perspective”. Journal of Psychopharmacology. 27 (6): 479–496. doi:10.1177/0269881113482532. PMC 3666194. PMID 23539642.
The intravenous use of d-amphetamine and other stimulants still pose major safety risks to the individuals indulging in this practice. Some of this intravenous abuse is derived from the diversion of ampoules of d-amphetamine, which are still occasionally prescribed in the UK for the control of severe narcolepsy and other disorders of excessive sedation. ... For these reasons, observations of dependence and abuse of prescription d-amphetamine are rare in clinical practice, and this stimulant can even be prescribed to people with a history of drug abuse provided certain controls, such as daily pick-ups of prescriptions, are put in place (Jasinski and Krishnan, 2009b).
Lỗi chú thích: Thẻ<ref>không hợp lệ: tên “Amph Uses” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ a b c d e f g h i j k l m n o p q “Adderall XR Prescribing Information” (PDF). United States Food and Drug Administration. Shire US Inc. tháng 12 năm 2013. tr. 12–13. Truy cập ngày 30 tháng 12 năm 2013.
- ^ a b c d e f Glennon RA (2013). “Phenylisopropylamine stimulants: amphetamine-related agents”. Trong Lemke TL, Williams DA, Roche VF, Zito W (biên tập). Foye's principles of medicinal chemistry (ấn bản 7). Philadelphia, USA: Wolters Kluwer Health/Lippincott Williams & Wilkins. tr. 646–648. ISBN 9781609133450.
The simplest unsubstituted phenylisopropylamine, 1-phenyl-2-aminopropane, or amphetamine, serves as a common structural template for hallucinogens and psychostimulants. Amphetamine produces central stimulant, anorectic, and sympathomimetic actions, and it is the prototype member of this class (39). ... The phase 1 metabolism of amphetamine analogs is catalyzed by two systems: cytochrome P450 and flavin monooxygenase. ... Amphetamine can also undergo aromatic hydroxylation to p-hydroxyamphetamine. ... Subsequent oxidation at the benzylic position by DA β-hydroxylase affords p-hydroxynorephedrine. Alternatively, direct oxidation of amphetamine by DA β-hydroxylase can afford norephedrine.
- ^ a b c Taylor KB (tháng 1 năm 1974). “Dopamine-beta-hydroxylase. Stereochemical course of the reaction” (PDF). Journal of Biological Chemistry. 249 (2): 454–458. PMID 4809526. Truy cập ngày 6 tháng 11 năm 2014.
Dopamine-β-hydroxylase catalyzed the removal of the pro-R hydrogen atom and the production of 1-norephedrine, (2S,1R)-2-amino-1-hydroxyl-1-phenylpropane, from d-amphetamine.
- ^ a b c Krueger SK, Williams DE (tháng 6 năm 2005). “Mammalian flavin-containing monooxygenases: structure/function, genetic polymorphisms and role in drug metabolism”. Pharmacology & Therapeutics. 106 (3): 357–387. doi:10.1016/j.pharmthera.2005.01.001. PMC 1828602. PMID 15922018.
Table 5: N-containing drugs and xenobiotics oxygenated by FMO - ^ a b c Cashman JR, Xiong YN, Xu L, Janowsky A (tháng 3 năm 1999). “N-oxygenation of amphetamine and methamphetamine by the human flavin-containing monooxygenase (form 3): role in bioactivation and detoxication”. Journal of Pharmacology and Experimental Therapeutics. 288 (3): 1251–1260. PMID 10027866.
- ^ Lỗi chú thích: Thẻ
<ref>sai; không có nội dung trong thẻ ref có tênDrugbank-dexamph - ^ a b c d Lỗi chú thích: Thẻ
<ref>sai; không có nội dung trong thẻ ref có tênDrugbank-amph - ^ a b c d e Santagati NA, Ferrara G, Marrazzo A, Ronsisvalle G (tháng 9 năm 2002). “Simultaneous determination of amphetamine and one of its metabolites by HPLC with electrochemical detection”. Journal of Pharmaceutical and Biomedical Analysis. 30 (2): 247–255. doi:10.1016/S0731-7085(02)00330-8. PMID 12191709.
- ^ “Pharmacology”. amphetamine/dextroamphetamine. Medscape. WebMD. Truy cập ngày 21 tháng 1 năm 2016.
Onset of action: 30–60 min
- ^ a b c Millichap JG (2010). “Chapter 9: Medications for ADHD”. Trong Millichap JG (biên tập). Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD (ấn bản 2). New York: Springer. tr. 112. ISBN 9781441913968.
Table 9.2 Dextroamphetamine formulations of stimulant medication
Dexedrine [Peak:2–3 h] [Duration:5–6 h] ...
Adderall [Peak:2–3 h] [Duration:5–7 h]
Dexedrine spansules [Peak:7–8 h] [Duration:12 h] ...
Adderall XR [Peak:7–8 h] [Duration:12 h]
Vyvanse [Peak:3–4 h] [Duration:12 h] - ^ Brams M, Mao AR, Doyle RL (tháng 9 năm 2008). “Onset of efficacy of long-acting psychostimulants in pediatric attention-deficit/hyperactivity disorder”. Postgraduate Medicine. 120 (3): 69–88. doi:10.3810/pgm.2008.09.1909. PMID 18824827. S2CID 31791162.
- ^ a b c d “Adderall- dextroamphetamine saccharate, amphetamine aspartate, dextroamphetamine sulfate, and amphetamine sulfate tablet”. DailyMed. Teva Pharmaceuticals USA, Inc. 8 tháng 11 năm 2019. Truy cập ngày 22 tháng 12 năm 2019.
- ^ a b c d e f Amphetamine. Hazardous Substances Data Bank. Bản gốc lưu trữ ngày 2 tháng 10 năm 2017. Truy cập ngày 2 tháng 10 năm 2017.
Duration of effect varies depending on agent and urine pH. Excretion is enhanced in more acidic urine. Half-life is 7 to 34 hours and is, in part, dependent on urine pH (half-life is longer with alkaline urine). ... Amphetamines are distributed into most body tissues with high concentrations occurring in the brain and CSF. Amphetamine appears in the urine within about 3 hours following oral administration. ... Three days after a dose of (+ or -)-amphetamine, human subjects had excreted 91% of the (14)C in the urine
- ^ a b Mignot EJ (tháng 10 năm 2012). “A practical guide to the therapy of narcolepsy and hypersomnia syndromes”. Neurotherapeutics. 9 (4): 739–752. doi:10.1007/s13311-012-0150-9. PMC 3480574. PMID 23065655.
- ^ “Density”. Amphetamine. PubChem Compound Database. United States National Library of Medicine – National Center for Biotechnology Information. 5 tháng 11 năm 2016. Truy cập ngày 9 tháng 11 năm 2016.
- ^ “Properties: Predicted – EPISuite”. Amphetamine. ChemSpider. Royal Society of Chemistry. Truy cập ngày 6 tháng 11 năm 2013.
- ^ a b Amphetamine. United States National Library of Medicine – National Center for Biotechnology Information.
|ngày truy cập=cần|url=(trợ giúp) - ^ “Hãy coi Người nghiện ma túy là người bệnh”. www.molisa.gov.vn (bằng tiếng Anh). Truy cập ngày 16 tháng 4 năm 2022.
- ^ Yoshida T (1997). “Chapter 1: Use and Misuse of Amphetamines: An International Overview”. Trong Klee H (biên tập). Amphetamine Misuse: International Perspectives on Current Trends. Amsterdam, Netherlands: Harwood Academic Publishers. tr. 2. ISBN 9789057020810.
Amphetamine, in the singular form, properly applies to the racemate of 2-amino-1-phenylpropane. ... In its broadest context, however, the term [amphetamines] can even embrace a large number of structurally and pharmacologically related substances.
- ^ a b c d e f g h i j Malenka RC, Nestler EJ, Hyman SE (2009). “Chapter 13: Higher Cognitive Function and Behavioral Control”. Trong Sydor A, Brown RY (biên tập). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (ấn bản 2). New York, USA: McGraw-Hill Medical. tr. 318, 321. ISBN 9780071481274.
Therapeutic (relatively low) doses of psychostimulants, such as methylphenidate and amphetamine, improve performance on working memory tasks both in normal subjects and those with ADHD. ... stimulants act not only on working memory function, but also on general levels of arousal and, within the nucleus accumbens, improve the saliency of tasks. Thus, stimulants improve performance on effortful but tedious tasks ... through indirect stimulation of dopamine and norepinephrine receptors. ...
Lỗi chú thích: Thẻ
Beyond these general permissive effects, dopamine (acting via D1 receptors) and norepinephrine (acting at several receptors) can, at optimal levels, enhance working memory and aspects of attention.<ref>không hợp lệ: tên “Malenka_2009” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ a b Lỗi chú thích: Thẻ
<ref>sai; không có nội dung trong thẻ ref có tênErgogenics - ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah ai aj “Adderall XR- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine sulfate and amphetamine aspartate capsule, extended release”. DailyMed. Shire US Inc. 17 tháng 7 năm 2019. Truy cập ngày 22 tháng 12 năm 2019.
- ^ a b c d Rasmussen N (tháng 7 năm 2006). “Making the first anti-depressant: amphetamine in American medicine, 1929–1950”. Journal of the History of Medicine and Allied Sciences. 61 (3): 288–323. doi:10.1093/jhmas/jrj039. PMID 16492800.
However the firm happened to discover the drug, SKF first packaged it as an inhaler so as to exploit the base's volatility and, after sponsoring some trials by East Coast otolaryngological specialists, began to advertise the Benzedrine Inhaler as a decongestant in late 1933.
- ^ a b “Convention on psychotropic substances”. United Nations Treaty Collection. United Nations. Lưu trữ bản gốc ngày 31 tháng 3 năm 2016. Truy cập ngày 11 tháng 11 năm 2013.
- ^ Lỗi chú thích: Thẻ
<ref>sai; không có nội dung trong thẻ ref có tênNonmedical - ^ a b Lỗi chú thích: Thẻ
<ref>sai; không có nội dung trong thẻ ref có tênLibido - ^ “Amphetamine”. Medical Subject Headings. United States National Library of Medicine. Truy cập ngày 16 tháng 12 năm 2013.
- ^ “Guidelines on the Use of International Nonproprietary Names (INNS) for Pharmaceutical Substances”. World Health Organization. 1997. Bản gốc lưu trữ ngày 9 tháng 1 năm 2015. Truy cập ngày 1 tháng 12 năm 2014.
In principle, INNs are selected only for the active part of the molecule which is usually the base, acid or alcohol. In some cases, however, the active molecules need to be expanded for various reasons, such as formulation purposes, bioavailability or absorption rate. In 1975 the experts designated for the selection of INN decided to adopt a new policy for naming such molecules. In future, names for different salts or esters of the same active substance should differ only with regard to the inactive moiety of the molecule. ... The latter are called modified INNs (INNMs).
- ^ a b c d e f g h i “Evekeo- amphetamine sulfate tablet”. DailyMed. Arbor Pharmaceuticals, LLC. 14 tháng 8 năm 2019. Truy cập ngày 22 tháng 12 năm 2019.
- ^ “National Drug Code Amphetamine Search Results”. National Drug Code Directory. United States Food and Drug Administration. Bản gốc lưu trữ ngày 16 tháng 12 năm 2013. Truy cập ngày 16 tháng 12 năm 2013.
- ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah Miller GM (tháng 1 năm 2011). “The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity”. Journal of Neurochemistry. 116 (2): 164–176. doi:10.1111/j.1471-4159.2010.07109.x. PMC 3005101. PMID 21073468.
- ^ a b c d e Grandy DK, Miller GM, Li JX (tháng 2 năm 2016). “"TAARgeting Addiction"-The Alamo Bears Witness to Another Revolution: An Overview of the Plenary Symposium of the 2015 Behavior, Biology and Chemistry Conference”. Drug and Alcohol Dependence. 159: 9–16. doi:10.1016/j.drugalcdep.2015.11.014. PMC 4724540. PMID 26644139.
When considered together with the rapidly growing literature in the field a compelling case emerges in support of developing TAAR1-selective agonists as medications for preventing relapse to psychostimulant abuse.
- ^ a b c d e f g h i j k l m n o p q r s t Westfall DP, Westfall TC (2010). “Miscellaneous Sympathomimetic Agonists”. Trong Brunton LL, Chabner BA, Knollmann BC (biên tập). Goodman & Gilman's Pharmacological Basis of Therapeutics (ấn bản 12). New York, USA: McGraw-Hill. ISBN 9780071624428.
- ^ Lỗi chú thích: Thẻ
<ref>sai; không có nội dung trong thẻ ref có tênCochrane - ^ a b c d e Bramness JG, Gundersen ØH, Guterstam J, Rognli EB, Konstenius M, Løberg EM, Medhus S, Tanum L, Franck J (tháng 12 năm 2012). “Amphetamine-induced psychosis—a separate diagnostic entity or primary psychosis triggered in the vulnerable?”. BMC Psychiatry. 12: 221. doi:10.1186/1471-244X-12-221. PMC 3554477. PMID 23216941.
In these studies, amphetamine was given in consecutively higher doses until psychosis was precipitated, often after 100–300 mg of amphetamine ... Secondly, psychosis has been viewed as an adverse event, although rare, in children with ADHD who have been treated with amphetamine
- ^ a b c Greydanus D. “Stimulant Misuse: Strategies to Manage a Growing Problem” (PDF). American College Health Association (Review Article). ACHA Professional Development Program. tr. 20. Bản gốc (PDF) lưu trữ ngày 3 tháng 11 năm 2013. Truy cập ngày 2 tháng 11 năm 2013.
- ^ a b c d e f g Huang YS, Tsai MH (tháng 7 năm 2011). “Long-term outcomes with medications for attention-deficit hyperactivity disorder: current status of knowledge”. CNS Drugs. 25 (7): 539–554. doi:10.2165/11589380-000000000-00000. PMID 21699268.
Several other studies,[97-101] including a meta-analytic review[98] and a retrospective study,[97] suggested that stimulant therapy in childhood is associated with a reduced risk of subsequent substance use, cigarette smoking and alcohol use disorders. ... Recent studies have demonstrated that stimulants, along with the non-stimulants atomoxetine and extended-release guanfacine, are continuously effective for more than 2-year treatment periods with few and tolerable adverse effects. The effectiveness of long-term therapy includes not only the core symptoms of ADHD, but also improved quality of life and academic achievements. The most concerning short-term adverse effects of stimulants, such as elevated blood pressure and heart rate, waned in long-term follow-up studies. ... The current data do not support the potential impact of stimulants on the worsening or development of tics or substance abuse into adulthood. In the longest follow-up study (of more than 10 years), lifetime stimulant treatment for ADHD was effective and protective against the development of adverse psychiatric disorders.
- ^ a b Malenka RC, Nestler EJ, Hyman SE, Holtzman DM (2015). “Chapter 16: Reinforcement and Addictive Disorders”. Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (ấn bản 3). New York: McGraw-Hill Medical. ISBN 9780071827706.
Such agents also have important therapeutic uses; cocaine, for example, is used as a local anesthetic (Chapter 2), and amphetamines and methylphenidate are used in low doses to treat attention deficit hyperactivity disorder and in higher doses to treat narcolepsy (Chapter 12). Despite their clinical uses, these drugs are strongly reinforcing, and their long-term use at high doses is linked with potential addiction, especially when they are rapidly administered or when high-potency forms are given.
- ^ a b Kollins SH (tháng 5 năm 2008). “A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders”. Current Medical Research and Opinion. 24 (5): 1345–1357. doi:10.1185/030079908X280707. PMID 18384709.
When oral formulations of psychostimulants are used at recommended doses and frequencies, they are unlikely to yield effects consistent with abuse potential in patients with ADHD.
- ^ a b Bett WR (tháng 8 năm 1946). “Benzedrine sulphate in clinical medicine; a survey of the literature”. Postgraduate Medical Journal. 22 (250): 205–218. doi:10.1136/pgmj.22.250.205. PMC 2478360. PMID 20997404.
- ^ Carvalho M, Carmo H, Costa VM, Capela JP, Pontes H, Remião F, Carvalho F, Bastos Mde L (tháng 8 năm 2012). “Toxicity of amphetamines: an update”. Archives of Toxicology. 86 (8): 1167–1231. doi:10.1007/s00204-012-0815-5. PMID 22392347.
- ^ Berman S, O'Neill J, Fears S, Bartzokis G, London ED (tháng 10 năm 2008). “Abuse of amphetamines and structural abnormalities in the brain”. Annals of the New York Academy of Sciences. 1141 (1): 195–220. doi:10.1196/annals.1441.031. PMC 2769923. PMID 18991959.
- ^ a b Hart H, Radua J, Nakao T, Mataix-Cols D, Rubia K (tháng 2 năm 2013). “Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: exploring task-specific, stimulant medication, and age effects”. JAMA Psychiatry. 70 (2): 185–198. doi:10.1001/jamapsychiatry.2013.277. PMID 23247506.
- ^ a b Spencer TJ, Brown A, Seidman LJ, Valera EM, Makris N, Lomedico A, Faraone SV, Biederman J (tháng 9 năm 2013). “Effect of psychostimulants on brain structure and function in ADHD: a qualitative literature review of magnetic resonance imaging-based neuroimaging studies”. The Journal of Clinical Psychiatry. 74 (9): 902–917. doi:10.4088/JCP.12r08287. PMC 3801446. PMID 24107764.
- ^ a b Frodl T, Skokauskas N (tháng 2 năm 2012). “Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects”. Acta Psychiatrica Scandinavica. 125 (2): 114–126. doi:10.1111/j.1600-0447.2011.01786.x. PMID 22118249.
Basal ganglia regions like the right globus pallidus, the right putamen, and the nucleus caudatus are structurally affected in children with ADHD. These changes and alterations in limbic regions like ACC and amygdala are more pronounced in non-treated populations and seem to diminish over time from child to adulthood. Treatment seems to have positive effects on brain structure.
- ^ a b c Millichap JG (2010). “Chapter 9: Medications for ADHD”. Trong Millichap JG (biên tập). Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD (ấn bản 2). New York, USA: Springer. tr. 121–123, 125–127. ISBN 9781441913968.
Ongoing research has provided answers to many of the parents' concerns, and has confirmed the effectiveness and safety of the long-term use of medication.
- ^ a b c d e Arnold LE, Hodgkins P, Caci H, Kahle J, Young S (tháng 2 năm 2015). “Effect of treatment modality on long-term outcomes in attention-deficit/hyperactivity disorder: a systematic review”. PLOS ONE. 10 (2): e0116407. doi:10.1371/journal.pone.0116407. PMC 4340791. PMID 25714373.
The highest proportion of improved outcomes was reported with combination treatment (83% of outcomes). Among significantly improved outcomes, the largest effect sizes were found for combination treatment. The greatest improvements were associated with academic, self-esteem, or social function outcomes.
Figure 3: Treatment benefit by treatment type and outcome group - ^ a b c Malenka RC, Nestler EJ, Hyman SE (2009). “Chapter 6: Widely Projecting Systems: Monoamines, Acetylcholine, and Orexin”. Trong Sydor A, Brown RY (biên tập). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (ấn bản 2). New York, USA: McGraw-Hill Medical. tr. 154–157. ISBN 9780071481274.
- ^ a b c d e Bidwell LC, McClernon FJ, Kollins SH (tháng 8 năm 2011). “Cognitive enhancers for the treatment of ADHD”. Pharmacology Biochemistry and Behavior. 99 (2): 262–274. doi:10.1016/j.pbb.2011.05.002. PMC 3353150. PMID 21596055.
- ^ Parker J, Wales G, Chalhoub N, Harpin V (tháng 9 năm 2013). “The long-term outcomes of interventions for the management of attention-deficit hyperactivity disorder in children and adolescents: a systematic review of randomized controlled trials”. Psychology Research and Behavior Management. 6: 87–99. doi:10.2147/PRBM.S49114. PMC 3785407. PMID 24082796.
Only one paper53 examining outcomes beyond 36 months met the review criteria. ... There is high level evidence suggesting that pharmacological treatment can have a major beneficial effect on the core symptoms of ADHD (hyperactivity, inattention, and impulsivity) in approximately 80% of cases compared with placebo controls, in the short term.
- ^ Millichap JG (2010). “Chapter 9: Medications for ADHD”. Trong Millichap JG (biên tập). Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD (ấn bản 2). New York, USA: Springer. tr. 111–113. ISBN 9781441913968.
- ^ “Stimulants for Attention Deficit Hyperactivity Disorder”. WebMD. Healthwise. 12 tháng 4 năm 2010. Truy cập ngày 12 tháng 11 năm 2013.
- ^ a b Castells X, Blanco-Silvente L, Cunill R (tháng 8 năm 2018). “Amphetamines for attention deficit hyperactivity disorder (ADHD) in adults”. Cochrane Database of Systematic Reviews. 2018 (8): CD007813. doi:10.1002/14651858.CD007813.pub3. PMC 6513464. PMID 30091808.
- ^ Punja S, Shamseer L, Hartling L, Urichuk L, Vandermeer B, Nikles J, Vohra S (tháng 2 năm 2016). “Amphetamines for attention deficit hyperactivity disorder (ADHD) in children and adolescents”. Cochrane Database of Systematic Reviews. 2: CD009996. doi:10.1002/14651858.CD009996.pub2. PMID 26844979.
- ^ Osland ST, Steeves TD, Pringsheim T (tháng 6 năm 2018). “Pharmacological treatment for attention deficit hyperactivity disorder (ADHD) in children with comorbid tic disorders”. Cochrane Database of Systematic Reviews. 2018 (6): CD007990. doi:10.1002/14651858.CD007990.pub3. PMC 6513283. PMID 29944175.
- ^ a b Spencer RC, Devilbiss DM, Berridge CW (tháng 6 năm 2015). “The Cognition-Enhancing Effects of Psychostimulants Involve Direct Action in the Prefrontal Cortex”. Biological Psychiatry. 77 (11): 940–950. doi:10.1016/j.biopsych.2014.09.013. PMC 4377121. PMID 25499957.
The procognitive actions of psychostimulants are only associated with low doses. Surprisingly, despite nearly 80 years of clinical use, the neurobiology of the procognitive actions of psychostimulants has only recently been systematically investigated. Findings from this research unambiguously demonstrate that the cognition-enhancing effects of psychostimulants involve the preferential elevation of catecholamines in the PFC and the subsequent activation of norepinephrine α2 and dopamine D1 receptors. ... This differential modulation of PFC-dependent processes across dose appears to be associated with the differential involvement of noradrenergic α2 versus α1 receptors. Collectively, this evidence indicates that at low, clinically relevant doses, psychostimulants are devoid of the behavioral and neurochemical actions that define this class of drugs and instead act largely as cognitive enhancers (improving PFC-dependent function). ... In particular, in both animals and humans, lower doses maximally improve performance in tests of working memory and response inhibition, whereas maximal suppression of overt behavior and facilitation of attentional processes occurs at higher doses.
- ^ Ilieva IP, Hook CJ, Farah MJ (tháng 6 năm 2015). “Prescription Stimulants' Effects on Healthy Inhibitory Control, Working Memory, and Episodic Memory: A Meta-analysis”. Journal of Cognitive Neuroscience. 27 (6): 1069–1089. doi:10.1162/jocn_a_00776. PMID 25591060.
Specifically, in a set of experiments limited to high-quality designs, we found significant enhancement of several cognitive abilities. ... The results of this meta-analysis ... do confirm the reality of cognitive enhancing effects for normal healthy adults in general, while also indicating that these effects are modest in size.
- ^ Bagot KS, Kaminer Y (tháng 4 năm 2014). “Efficacy of stimulants for cognitive enhancement in non-attention deficit hyperactivity disorder youth: a systematic review”. Addiction. 109 (4): 547–557. doi:10.1111/add.12460. PMC 4471173. PMID 24749160.
Amphetamine has been shown to improve consolidation of information (0.02 ≥ P ≤ 0.05), leading to improved recall.
- ^ Devous MD, Trivedi MH, Rush AJ (tháng 4 năm 2001). “Regional cerebral blood flow response to oral amphetamine challenge in healthy volunteers”. Journal of Nuclear Medicine. 42 (4): 535–542. PMID 11337538.
- ^ Malenka RC, Nestler EJ, Hyman SE (2009). “Chapter 10: Neural and Neuroendocrine Control of the Internal Milieu”. Trong Sydor A, Brown RY (biên tập). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (ấn bản 2). New York, USA: McGraw-Hill Medical. tr. 266. ISBN 9780071481274.
Dopamine acts in the nucleus accumbens to attach motivational significance to stimuli associated with reward.
- ^ a b c Wood S, Sage JR, Shuman T, Anagnostaras SG (tháng 1 năm 2014). “Psychostimulants and cognition: a continuum of behavioral and cognitive activation”. Pharmacological Reviews. 66 (1): 193–221. doi:10.1124/pr.112.007054. PMC 3880463. PMID 24344115.
- ^ Twohey M (26 tháng 3 năm 2006). “Pills become an addictive study aid”. JS Online. Bản gốc lưu trữ ngày 15 tháng 8 năm 2007. Truy cập ngày 2 tháng 12 năm 2007.
- ^ Teter CJ, McCabe SE, LaGrange K, Cranford JA, Boyd CJ (tháng 10 năm 2006). “Illicit use of specific prescription stimulants among college students: prevalence, motives, and routes of administration”. Pharmacotherapy. 26 (10): 1501–1510. doi:10.1592/phco.26.10.1501. PMC 1794223. PMID 16999660.
- ^ Weyandt LL, Oster DR, Marraccini ME, Gudmundsdottir BG, Munro BA, Zavras BM, Kuhar B (tháng 9 năm 2014). “Pharmacological interventions for adolescents and adults with ADHD: stimulant and nonstimulant medications and misuse of prescription stimulants”. Psychology Research and Behavior Management. 7: 223–249. doi:10.2147/PRBM.S47013. PMC 4164338. PMID 25228824.
misuse of prescription stimulants has become a serious problem on college campuses across the US and has been recently documented in other countries as well. ... Indeed, large numbers of students claim to have engaged in the nonmedical use of prescription stimulants, which is reflected in lifetime prevalence rates of prescription stimulant misuse ranging from 5% to nearly 34% of students.
- ^ Clemow DB, Walker DJ (tháng 9 năm 2014). “The potential for misuse and abuse of medications in ADHD: a review”. Postgraduate Medicine. 126 (5): 64–81. doi:10.3810/pgm.2014.09.2801. PMID 25295651.
Overall, the data suggest that ADHD medication misuse and diversion are common health care problems for stimulant medications, with the prevalence believed to be approximately 5% to 10% of high school students and 5% to 35% of college students, depending on the study.
- ^ Bracken NM (tháng 1 năm 2012). “National Study of Substance Use Trends Among NCAA College Student-Athletes” (PDF). NCAA Publications. National Collegiate Athletic Association. Lưu trữ (PDF) bản gốc ngày 9 tháng 10 năm 2022. Truy cập ngày 8 tháng 10 năm 2013.
- ^ Docherty JR (tháng 6 năm 2008). “Pharmacology of stimulants prohibited by the World Anti-Doping Agency (WADA)”. British Journal of Pharmacology. 154 (3): 606–622. doi:10.1038/bjp.2008.124. PMC 2439527. PMID 18500382.
- ^ a b c d Parr JW (tháng 7 năm 2011). “Attention-deficit hyperactivity disorder and the athlete: new advances and understanding”. Clinics in Sports Medicine. 30 (3): 591–610. doi:10.1016/j.csm.2011.03.007. PMID 21658550.
In 1980, Chandler and Blair47 showed significant increases in knee extension strength, acceleration, anaerobic capacity, time to exhaustion during exercise, pre-exercise and maximum heart rates, and time to exhaustion during maximal oxygen consumption (VO2 max) testing after administration of 15 mg of dextroamphetamine versus placebo. Most of the information to answer this question has been obtained in the past decade through studies of fatigue rather than an attempt to systematically investigate the effect of ADHD drugs on exercise.
- ^ a b c Roelands B, de Koning J, Foster C, Hettinga F, Meeusen R (tháng 5 năm 2013). “Neurophysiological determinants of theoretical concepts and mechanisms involved in pacing”. Sports Medicine. 43 (5): 301–311. doi:10.1007/s40279-013-0030-4. PMID 23456493.
In high-ambient temperatures, dopaminergic manipulations clearly improve performance. The distribution of the power output reveals that after dopamine reuptake inhibition, subjects are able to maintain a higher power output compared with placebo. ... Dopaminergic drugs appear to override a safety switch and allow athletes to use a reserve capacity that is 'off-limits' in a normal (placebo) situation.
- ^ Parker KL, Lamichhane D, Caetano MS, Narayanan NS (tháng 10 năm 2013). “Executive dysfunction in Parkinson's disease and timing deficits”. Frontiers in Integrative Neuroscience. 7: 75. doi:10.3389/fnint.2013.00075. PMC 3813949. PMID 24198770.
Manipulations of dopaminergic signaling profoundly influence interval timing, leading to the hypothesis that dopamine influences internal pacemaker, or "clock," activity. For instance, amphetamine, which increases concentrations of dopamine at the synaptic cleft advances the start of responding during interval timing, whereas antagonists of D2 type dopamine receptors typically slow timing;... Depletion of dopamine in healthy volunteers impairs timing, while amphetamine releases synaptic dopamine and speeds up timing.
- ^ Rattray B, Argus C, Martin K, Northey J, Driller M (tháng 3 năm 2015). “Is it time to turn our attention toward central mechanisms for post-exertional recovery strategies and performance?”. Frontiers in Physiology. 6: 79. doi:10.3389/fphys.2015.00079. PMC 4362407. PMID 25852568.
Aside from accounting for the reduced performance of mentally fatigued participants, this model rationalizes the reduced RPE and hence improved cycling time trial performance of athletes using a glucose mouthwash (Chambers et al., 2009) and the greater power output during a RPE matched cycling time trial following amphetamine ingestion (Swart, 2009). ... Dopamine stimulating drugs are known to enhance aspects of exercise performance (Roelands et al., 2008)
- ^ Roelands B, De Pauw K, Meeusen R (tháng 6 năm 2015). “Neurophysiological effects of exercise in the heat”. Scandinavian Journal of Medicine & Science in Sports. 25 (Suppl 1): 65–78. doi:10.1111/sms.12350. PMID 25943657.
This indicates that subjects did not feel they were producing more power and consequently more heat. The authors concluded that the "safety switch" or the mechanisms existing in the body to prevent harmful effects are overridden by the drug administration (Roelands et al., 2008b). Taken together, these data indicate strong ergogenic effects of an increased DA concentration in the brain, without any change in the perception of effort.
- ^ Feinberg SS (tháng 11 năm 2004). “Combining stimulants with monoamine oxidase inhibitors: a review of uses and one possible additional indication”. The Journal of Clinical Psychiatry. 65 (11): 1520–1524. doi:10.4088/jcp.v65n1113. PMID 15554766.
- ^ Stewart JW, Deliyannides DA, McGrath PJ (tháng 6 năm 2014). “How treatable is refractory depression?”. Journal of Affective Disorders. 167: 148–152. doi:10.1016/j.jad.2014.05.047. PMID 24972362.
- ^ Vitiello B (tháng 4 năm 2008). “Understanding the risk of using medications for attention deficit hyperactivity disorder with respect to physical growth and cardiovascular function”. Child and Adolescent Psychiatric Clinics of North America. 17 (2): 459–474. doi:10.1016/j.chc.2007.11.010. PMC 2408826. PMID 18295156.
- ^ Thuật ngữ lấy từ:[https://mlearning.hoasen.edu.vn/pluginfile.php/60438/mod_resource/content/1/Ba%CC%80i%203%20-%20%C4%90ie%CC%82%CC%80u%20kie%CC%A3%CC%82n%20hoa%CC%81%20pha%CC%89n%20ho%CC%82%CC%80i.pdf]
- ^ a b Childs E, de Wit H (tháng 5 năm 2009). “Amphetamine-induced place preference in humans”. Biological Psychiatry. 65 (10): 900–904. doi:10.1016/j.biopsych.2008.11.016. PMC 2693956. PMID 19111278.
This study demonstrates that humans, like nonhumans, prefer a place associated with amphetamine administration. These findings support the idea that subjective responses to a drug contribute to its ability to establish place conditioning.
- ^ Malenka RC, Nestler EJ, Hyman SE (2009). “Chapter 15: Reinforcement and Addictive Disorders”. Trong Sydor A, Brown RY (biên tập). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (ấn bản 2). New York: McGraw-Hill Medical. tr. 364–375. ISBN 9780071481274.
- ^ Nestler EJ (tháng 12 năm 2013). “Cellular basis of memory for addiction”. Dialogues in Clinical Neuroscience. 15 (4): 431–443. PMC 3898681. PMID 24459410.
Mặc cho tầm quan trọng của nhiều yếu tố tâm lý xã hội, nhưng về bản chất, nghiện ma túy bao gồm một quá trình sinh học: khả năng tiếp xúc nhiều lần với một loại thuốc lạm dụng để tạo ra những thay đổi trong não dễ bị tổn thương dẫn tới việc kiếm tìm và uống thuốc mang tính bắt buộc, và mất khả năng kiểm soát việc sử dụng ma túy, điều xác định tình trạng nghiện. ... Một tài liệu lớn đã chứng minh rằng loại cảm ứng ΔFosB như vậy trong các tế bào thần kinh loại D1 [nhân cạp - nucleus accumbens] làm tăng độ nhạy cảm của động vật đối với ma túy cũng như các phần thưởng tự nhiên và thúc đẩy việc tự cho phép sử dụng ma tùy, có lẽ thông qua quá trình củng cố tích cực ... Một mục tiêu ΔFosB khác là cFos: bởi ΔFosB tích lũy khi tiếp xúc với thuốc lặp đi lặp lại, nó ức chế c-Fos và góp phần chuyển đổi phân tử, theo đó ΔFosB được chọn lọc trong trạng thái điều trị ma túy mãn tính.41 ... Hơn nữa, ngày càng có nhiều bằng chứng cho thấy, mặc dù có nhiều rủi ro di truyền gây nghiện trong dân số, việc tiếp xúc với liều thuốc đủ cao trong thời gian dài có thể biến một người có tải lượng gen tương đối thấp thành con nghiện.
- ^ “Glossary of Terms”. Mount Sinai School of Medicine. Department of Neuroscience. Truy cập ngày 9 tháng 2 năm 2015.
- ^ Volkow ND, Koob GF, McLellan AT (tháng 1 năm 2016). “Neurobiologic Advances from the Brain Disease Model of Addiction”. New England Journal of Medicine. 374 (4): 363–371. doi:10.1056/NEJMra1511480. PMC 6135257. PMID 26816013.
Rối loạn sử dụng chất: Thuật ngữ chẩn đoán trong phiên bản thứ năm của Cẩm nang chẩn đoán và thống kê rối loạn tâm thần (DSM-5) đề cập đến việc sử dụng rượu hoặc các loại thuốc khác gây suy giảm đáng kể về mặt lâm sàng và chức năng, như các vấn đề về sức khỏe, khuyết tật, và không đáp ứng các trách nhiệm chính tại nơi làm việc, trường học hoặc nhà. Tùy thuộc vào mức độ nghiêm trọng, rối loạn này được phân loại là nhẹ, trung bình hoặc nặng.
Nghiện: Một thuật ngữ được sử dụng để chỉ giai đoạn rối loạn sử dụng chất nghiêm trọng và mãn tính nhất, trong đó có sự mất tự chủ đáng kể, được chỉ định bằng cách uống thuốc bắt buộc mặc dù muốn ngừng dùng thuốc. Trong DSM-5, thuật ngữ 'nghiện' đồng nghĩa với việc phân loại rối loạn sử dụng chất nghiêm trọng. - ^ a b c d e f Renthal W, Nestler EJ (tháng 9 năm 2009). “Chromatin regulation in drug addiction and depression”. Dialogues in Clinical Neuroscience. 11 (3): 257–268. PMC 2834246. PMID 19877494.
[Psychostimulants] increase cAMP levels in striatum, which activates protein kinase A (PKA) and leads to phosphorylation of its targets. This includes the cAMP response element binding protein (CREB), the phosphorylation of which induces its association with the histone acetyltransferase, CREB binding protein (CBP) to acetylate histones and facilitate gene activation. This is known to occur on many genes including fosB and c-fos in response to psychostimulant exposure. ΔFosB is also upregulated by chronic psychostimulant treatments, and is known to activate certain genes (eg, cdk5) and repress others (eg, c-fos) where it recruits HDAC1 as a corepressor. ... Chronic exposure to psychostimulants increases glutamatergic [signaling] from the prefrontal cortex to the NAc. Glutamatergic signaling elevates Ca2+ levels in NAc postsynaptic elements where it activates CaMK (calcium/calmodulin protein kinases) signaling, which, in addition to phosphorylating CREB, also phosphorylates HDAC5.
Figure 2: Psychostimulant-induced signaling events - ^ a b Broussard JI (tháng 1 năm 2012). “Co-transmission of dopamine and glutamate”. The Journal of General Physiology. 139 (1): 93–96. doi:10.1085/jgp.201110659. PMC 3250102. PMID 22200950.
Coincident and convergent input often induces plasticity on a postsynaptic neuron. The NAc integrates processed information about the environment from basolateral amygdala, hippocampus, and prefrontal cortex (PFC), as well as projections from midbrain dopamine neurons. Previous studies have demonstrated how dopamine modulates this integrative process. For example, high frequency stimulation potentiates hippocampal inputs to the NAc while simultaneously depressing PFC synapses (Goto and Grace, 2005). The converse was also shown to be true; stimulation at PFC potentiates PFC–NAc synapses but depresses hippocampal–NAc synapses. In light of the new functional evidence of midbrain dopamine/glutamate co-transmission (references above), new experiments of NAc function will have to test whether midbrain glutamatergic inputs bias or filter either limbic or cortical inputs to guide goal-directed behavior.
- ^ a b Kanehisa Laboratories (10 tháng 10 năm 2014). “Amphetamine – Homo sapiens (human)”. KEGG Pathway. Truy cập ngày 31 tháng 10 năm 2014.
Most addictive drugs increase extracellular concentrations of dopamine (DA) in nucleus accumbens (NAc) and medial prefrontal cortex (mPFC), projection areas of mesocorticolimbic DA neurons and key components of the "brain reward circuit". Amphetamine achieves this elevation in extracellular levels of DA by promoting efflux from synaptic terminals. ... Chronic exposure to amphetamine induces a unique transcription factor delta FosB, which plays an essential role in long-term adaptive changes in the brain.
- ^ a b Cadet JL, Brannock C, Jayanthi S, Krasnova IN (2015). “Transcriptional and epigenetic substrates of methamphetamine addiction and withdrawal: evidence from a long-access self-administration model in the rat”. Molecular Neurobiology. 51 (2): 696–717 (Figure 1). doi:10.1007/s12035-014-8776-8. PMC 4359351. PMID 24939695.
- ^ a b c d e f Robison AJ, Nestler EJ (tháng 11 năm 2011). “Transcriptional and epigenetic mechanisms of addiction”. Nature Reviews Neuroscience. 12 (11): 623–637. doi:10.1038/nrn3111. PMC 3272277. PMID 21989194.
ΔFosB serves as one of the master control proteins governing this structural plasticity. ... ΔFosB also represses G9a expression, leading to reduced repressive histone methylation at the cdk5 gene. The net result is gene activation and increased CDK5 expression. ... In contrast, ΔFosB binds to the c-fos gene and recruits several co-repressors, including HDAC1 (histone deacetylase 1) and SIRT 1 (sirtuin 1). ... The net result is c-fos gene repression.
Figure 4: Epigenetic basis of drug regulation of gene expression - ^ a b c d e f Nestler EJ (tháng 12 năm 2012). “Transcriptional mechanisms of drug addiction”. Clinical Psychopharmacology and Neuroscience. 10 (3): 136–143. doi:10.9758/cpn.2012.10.3.136. PMC 3569166. PMID 23430970.
The 35-37 kD ΔFosB isoforms accumulate with chronic drug exposure due to their extraordinarily long half-lives. ... As a result of its stability, the ΔFosB protein persists in neurons for at least several weeks after cessation of drug exposure. ... ΔFosB overexpression in nucleus accumbens induces NFκB ... In contrast, the ability of ΔFosB to repress the c-Fos gene occurs in concert with the recruitment of a histone deacetylase and presumably several other repressive proteins such as a repressive histone methyltransferase
- ^ a b Nestler EJ (tháng 10 năm 2008). “Transcriptional mechanisms of addiction: Role of ΔFosB”. Philosophical Transactions of the Royal Society B: Biological Sciences. 363 (1507): 3245–3255. doi:10.1098/rstb.2008.0067. PMC 2607320. PMID 18640924.
Recent evidence has shown that ΔFosB also represses the c-fos gene that helps create the molecular switch—from the induction of several short-lived Fos family proteins after acute drug exposure to the predominant accumulation of ΔFosB after chronic drug exposure
- ^ Kanehisa Laboratories (10 tháng 10 năm 2014). “Amphetamine – Homo sapiens (human)”. KEGG Pathway. Truy cập ngày 31 tháng 10 năm 2014.
- ^ a b c d Nechifor M (tháng 3 năm 2008). “Magnesium in drug dependences”. Magnesium Research. 21 (1): 5–15. doi:10.1684/mrh.2008.0124 (không hoạt động 31 July 2022). PMID 18557129.Quản lý CS1: DOI không hoạt động tính đến tháng 7 2022 (liên kết) Lỗi chú thích: Thẻ
<ref>không hợp lệ: tên “Magnesium” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ a b c d Ruffle JK (tháng 11 năm 2014). “Molecular neurobiology of addiction: what's all the (Δ)FosB about?”. The American Journal of Drug and Alcohol Abuse. 40 (6): 428–437. doi:10.3109/00952990.2014.933840. PMID 25083822.
ΔFosB is an essential transcription factor implicated in the molecular and behavioral pathways of addiction following repeated drug exposure.
- ^ a b c d e f g h i Robison AJ, Nestler EJ (tháng 11 năm 2011). “Transcriptional and epigenetic mechanisms of addiction”. Nature Reviews Neuroscience. 12 (11): 623–637. doi:10.1038/nrn3111. PMC 3272277. PMID 21989194.
ΔFosB has been linked directly to several addiction-related behaviors ... Importantly, genetic or viral overexpression of ΔJunD, a dominant negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure14,22–24. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high fat food, sex, wheel running, where it promotes that consumption14,26–30. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states. ... ΔFosB serves as one of the master control proteins governing this structural plasticity.
Lỗi chú thích: Thẻ<ref>không hợp lệ: tên “Nestler” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ a b c d e f g Olsen CM (tháng 12 năm 2011). “Natural rewards, neuroplasticity, and non-drug addictions”. Neuropharmacology. 61 (7): 1109–1122. doi:10.1016/j.neuropharm.2011.03.010. PMC 3139704. PMID 21459101.
Similar to environmental enrichment, studies have found that exercise reduces self-administration and relapse to drugs of abuse (Cosgrove et al., 2002; Zlebnik et al., 2010). There is also some evidence that these preclinical findings translate to human populations, as exercise reduces withdrawal symptoms and relapse in abstinent smokers (Daniel et al., 2006; Prochaska et al., 2008), and one drug recovery program has seen success in participants that train for and compete in a marathon as part of the program (Butler, 2005). ... In humans, the role of dopamine signaling in incentive-sensitization processes has recently been highlighted by the observation of a dopamine dysregulation syndrome in some patients taking dopaminergic drugs. This syndrome is characterized by a medication-induced increase in (or compulsive) engagement in non-drug rewards such as gambling, shopping, or sex (Evans et al., 2006; Aiken, 2007; Lader, 2008).
Lỗi chú thích: Thẻ<ref>không hợp lệ: tên “Natural and drug addictions” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ a b c Lynch WJ, Peterson AB, Sanchez V, Abel J, Smith MA (tháng 9 năm 2013). “Exercise as a novel treatment for drug addiction: a neurobiological and stage-dependent hypothesis”. Neuroscience & Biobehavioral Reviews. 37 (8): 1622–1644. doi:10.1016/j.neubiorev.2013.06.011. PMC 3788047. PMID 23806439.
These findings suggest that exercise may "magnitude"-dependently prevent the development of an addicted phenotype possibly by blocking/reversing behavioral and neuroadaptive changes that develop during and following extended access to the drug. ... Exercise has been proposed as a treatment for drug addiction that may reduce drug craving and risk of relapse. Although few clinical studies have investigated the efficacy of exercise for preventing relapse, the few studies that have been conducted generally report a reduction in drug craving and better treatment outcomes ... Taken together, these data suggest that the potential benefits of exercise during relapse, particularly for relapse to psychostimulants, may be mediated via chromatin remodeling and possibly lead to greater treatment outcomes.
- ^ a b Zhou Y, Zhao M, Zhou C, Li R (tháng 7 năm 2015). “Sex differences in drug addiction and response to exercise intervention: From human to animal studies”. Frontiers in Neuroendocrinology. 40: 24–41. doi:10.1016/j.yfrne.2015.07.001. PMC 4712120. PMID 26182835.
Collectively, these findings demonstrate that exercise may serve as a substitute or competition for drug abuse by changing ΔFosB or cFos immunoreactivity in the reward system to protect against later or previous drug use. ... The postulate that exercise serves as an ideal intervention for drug addiction has been widely recognized and used in human and animal rehabilitation.
- ^ a b Linke SE, Ussher M (tháng 1 năm 2015). “Exercise-based treatments for substance use disorders: evidence, theory, and practicality”. The American Journal of Drug and Alcohol Abuse. 41 (1): 7–15. doi:10.3109/00952990.2014.976708. PMC 4831948. PMID 25397661.
The limited research conducted suggests that exercise may be an effective adjunctive treatment for SUDs. In contrast to the scarce intervention trials to date, a relative abundance of literature on the theoretical and practical reasons supporting the investigation of this topic has been published. ... numerous theoretical and practical reasons support exercise-based treatments for SUDs, including psychological, behavioral, neurobiological, nearly universal safety profile, and overall positive health effects.
- ^ Hyman SE, Malenka RC, Nestler EJ (tháng 7 năm 2006). “Neural mechanisms of addiction: the role of reward-related learning and memory” (PDF). Annual Review of Neuroscience. 29: 565–598. doi:10.1146/annurev.neuro.29.051605.113009. PMID 16776597. Bản gốc (PDF) lưu trữ ngày 19 tháng 9 năm 2018.
- ^ a b c d e Steiner H, Van Waes V (tháng 1 năm 2013). “Addiction-related gene regulation: risks of exposure to cognitive enhancers vs. other psychostimulants”. Progress in Neurobiology. 100: 60–80. doi:10.1016/j.pneurobio.2012.10.001. PMC 3525776. PMID 23085425.
- ^ Xem cách sử dụng thuật ngữ tại [https://tapchiyhocvietnam.vn/index.php/vmj/article/view/54 Tạp chí Y học Việt Nam]
- ^ a b Nestler EJ (tháng 1 năm 2014). “Epigenetic mechanisms of drug addiction”. Neuropharmacology. 76 Pt B: 259–268. doi:10.1016/j.neuropharm.2013.04.004. PMC 3766384. PMID 23643695.
- ^ a b Blum K, Werner T, Carnes S, Carnes P, Bowirrat A, Giordano J, Oscar-Berman M, Gold M (tháng 3 năm 2012). “Sex, drugs, and rock 'n' roll: hypothesizing common mesolimbic activation as a function of reward gene polymorphisms”. Journal of Psychoactive Drugs. 44 (1): 38–55. doi:10.1080/02791072.2012.662112. PMC 4040958. PMID 22641964.
It has been found that deltaFosB gene in the NAc is critical for reinforcing effects of sexual reward. Pitchers and colleagues (2010) reported that sexual experience was shown to cause DeltaFosB accumulation in several limbic brain regions including the NAc, medial pre-frontal cortex, VTA, caudate, and putamen, but not the medial preoptic nucleus. ... these findings support a critical role for DeltaFosB expression in the NAc in the reinforcing effects of sexual behavior and sexual experience-induced facilitation of sexual performance. ... both drug addiction and sexual addiction represent pathological forms of neuroplasticity along with the emergence of aberrant behaviors involving a cascade of neurochemical changes mainly in the brain's rewarding circuitry.
- ^ Pitchers KK, Vialou V, Nestler EJ, Laviolette SR, Lehman MN, Coolen LM (tháng 2 năm 2013). “Natural and drug rewards act on common neural plasticity mechanisms with ΔFosB as a key mediator”. The Journal of Neuroscience. 33 (8): 3434–3442. doi:10.1523/JNEUROSCI.4881-12.2013. PMC 3865508. PMID 23426671.
- ^ Beloate LN, Weems PW, Casey GR, Webb IC, Coolen LM (tháng 2 năm 2016). “Nucleus accumbens NMDA receptor activation regulates amphetamine cross-sensitization and deltaFosB expression following sexual experience in male rats”. Neuropharmacology. 101: 154–164. doi:10.1016/j.neuropharm.2015.09.023. PMID 26391065.
- ^ Malenka RC, Nestler EJ, Hyman SE, Holtzman DM (2015). “Chapter 16: Reinforcement and Addictive Disorders”. Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (ấn bản 3). New York: McGraw-Hill Medical. ISBN 9780071827706.
Pharmacologic treatment for psychostimulant addiction is generally unsatisfactory. As previously discussed, cessation of cocaine use and the use of other psychostimulants in dependent individuals does not produce a physical withdrawal syndrome but may produce dysphoria, anhedonia, and an intense desire to reinitiate drug use.
- ^ a b c d Chan B, Freeman M, Kondo K, Ayers C, Montgomery J, Paynter R, Kansagara D (tháng 12 năm 2019). “Pharmacotherapy for methamphetamine/amphetamine use disorder-a systematic review and meta-analysis”. Addiction. 114 (12): 2122–2136. doi:10.1111/add.14755. PMID 31328345. Lỗi chú thích: Thẻ
<ref>không hợp lệ: tên “SystRev-Meta analysis amphetamine addiction pharmacotherapy” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ Stoops WW, Rush CR (tháng 5 năm 2014). “Combination pharmacotherapies for stimulant use disorder: a review of clinical findings and recommendations for future research”. Expert Review of Clinical Pharmacology. 7 (3): 363–374. doi:10.1586/17512433.2014.909283. PMC 4017926. PMID 24716825.
Despite concerted efforts to identify a pharmacotherapy for managing stimulant use disorders, no widely effective medications have been approved.
- ^ a b Jing L, Li JX (tháng 8 năm 2015). “Trace amine-associated receptor 1: A promising target for the treatment of psychostimulant addiction”. European Journal of Pharmacology. 761: 345–352. doi:10.1016/j.ejphar.2015.06.019. PMC 4532615. PMID 26092759.
Existing data provided robust preclinical evidence supporting the development of TAAR1 agonists as potential treatment for psychostimulant abuse and addiction.
- ^ Xem nội dung Chương trình 12 bước tại: [https://www.maihuong.gov.vn/vi/chuong-trinh-phong-chong-ma-tuy/tom-tat-chuong-trinh-dieu-tri-nghien-12-buoc-hoi-phuc.html trang web của bệnh viện tâm thần ban ngày Mai Hương]
- ^ a b Carroll ME, Smethells JR (tháng 2 năm 2016). “Sex Differences in Behavioral Dyscontrol: Role in Drug Addiction and Novel Treatments”. Frontiers in Psychiatry. 6: 175. doi:10.3389/fpsyt.2015.00175. PMC 4745113. PMID 26903885.
Physical Exercise
There is accelerating evidence that physical exercise is a useful treatment for preventing and reducing drug addiction ... In some individuals, exercise has its own rewarding effects, and a behavioral economic interaction may occur, such that physical and social rewards of exercise can substitute for the rewarding effects of drug abuse. ... The value of this form of treatment for drug addiction in laboratory animals and humans is that exercise, if it can substitute for the rewarding effects of drugs, could be self-maintained over an extended period of time. Work to date in [laboratory animals and humans] regarding exercise as a treatment for drug addiction supports this hypothesis. ... Animal and human research on physical exercise as a treatment for stimulant addiction indicates that this is one of the most promising treatments on the horizon. - ^ Perez-Mana C, Castells X, Torrens M, Capella D, Farre M (tháng 9 năm 2013). “Efficacy of psychostimulant drugs for amphetamine abuse or dependence”. Cochrane Database of Systematic Reviews. 9 (9): CD009695. doi:10.1002/14651858.CD009695.pub2. PMID 23996457.
- ^ “Amphetamines: Drug Use and Abuse”. Merck Manual Home Edition. Merck. tháng 2 năm 2003. Bản gốc lưu trữ ngày 17 tháng 2 năm 2007. Truy cập ngày 28 tháng 2 năm 2007.
- ^ a b c d Shoptaw SJ, Kao U, Heinzerling K, Ling W (tháng 4 năm 2009). “Treatment for amphetamine withdrawal”. Cochrane Database of Systematic Reviews (2): CD003021. doi:10.1002/14651858.CD003021.pub2. PMC 7138250. PMID 19370579.
The prevalence of this withdrawal syndrome is extremely common (Cantwell 1998; Gossop 1982) with 87.6% of 647 individuals with amphetamine dependence reporting six or more signs of amphetamine withdrawal listed in the DSM when the drug is not available (Schuckit 1999) ... The severity of withdrawal symptoms is greater in amphetamine dependent individuals who are older and who have more extensive amphetamine use disorders (McGregor 2005). Withdrawal symptoms typically present within 24 hours of the last use of amphetamine, with a withdrawal syndrome involving two general phases that can last 3 weeks or more. The first phase of this syndrome is the initial "crash" that resolves within about a week (Gossop 1982;McGregor 2005) ...
- ^ Spiller HA, Hays HL, Aleguas A (tháng 6 năm 2013). “Overdose of drugs for attention-deficit hyperactivity disorder: clinical presentation, mechanisms of toxicity, and management”. CNS Drugs. 27 (7): 531–543. doi:10.1007/s40263-013-0084-8. PMID 23757186.
Amphetamine, dextroamphetamine, and methylphenidate act as substrates for the cellular monoamine transporter, especially the dopamine transporter (DAT) and less so the norepinephrine (NET) and serotonin transporter. The mechanism of toxicity is primarily related to excessive extracellular dopamine, norepinephrine, and serotonin.
- ^ Collaborators (2015). “Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013”. The Lancet. 385 (9963): 117–171. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
Amphetamine use disorders ... 3,788 (3,425–4,145)
- ^ Advokat C (tháng 7 năm 2007). “Update on amphetamine neurotoxicity and its relevance to the treatment of ADHD”. Journal of Attention Disorders. 11 (1): 8–16. doi:10.1177/1087054706295605. PMID 17606768.
- ^ a b c Bowyer JF, Hanig JP (tháng 11 năm 2014). “Amphetamine- and methamphetamine-induced hyperthermia: Implications of the effects produced in brain vasculature and peripheral organs to forebrain neurotoxicity”. Temperature. 1 (3): 172–182. doi:10.4161/23328940.2014.982049. PMC 5008711. PMID 27626044.
Hyperthermia alone does not produce amphetamine-like neurotoxicity but AMPH and METH exposures that do not produce hyperthermia (≥40 °C) are minimally neurotoxic. Hyperthermia likely enhances AMPH and METH neurotoxicity directly through disruption of protein function, ion channels and enhanced ROS production. ... The hyperthermia and the hypertension produced by high doses amphetamines are a primary cause of transient breakdowns in the blood-brain barrier (BBB) resulting in concomitant regional neurodegeneration and neuroinflammation in laboratory animals. ... In animal models that evaluate the neurotoxicity of AMPH and METH, it is quite clear that hyperthermia is one of the essential components necessary for the production of histological signs of dopamine terminal damage and neurodegeneration in cortex, striatum, thalamus and hippocampus.
- ^ “Amphetamine”. United States National Library of Medicine – Toxicology Data Network. Hazardous Substances Data Bank. Bản gốc lưu trữ ngày 2 tháng 10 năm 2017. Truy cập ngày 2 tháng 10 năm 2017.
Direct toxic damage to vessels seems unlikely because of the dilution that occurs before the drug reaches the cerebral circulation.
- ^ Malenka RC, Nestler EJ, Hyman SE (2009). “Chapter 15: Reinforcement and addictive disorders”. Trong Sydor A, Brown RY (biên tập). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (ấn bản 2). New York, USA: McGraw-Hill Medical. tr. 370. ISBN 9780071481274.
Unlike cocaine and amphetamine, methamphetamine is directly toxic to midbrain dopamine neurons.
- ^ Thuật ngữ lấy từ[http://hoithankinhhocvietnam.com.vn/tham-luan-ve-goc-tu-do/ Tham luận về gốc tự do của Hội Thần kinh học Việt Nam]
- ^ Shoptaw SJ, Kao U, Ling W (tháng 1 năm 2009). Shoptaw SJ, Ali R (biên tập). “Treatment for amphetamine psychosis”. Cochrane Database of Systematic Reviews (1): CD003026. doi:10.1002/14651858.CD003026.pub3. PMC 7004251. PMID 19160215.
A minority of individuals who use amphetamines develop full-blown psychosis requiring care at emergency departments or psychiatric hospitals. In such cases, symptoms of amphetamine psychosis commonly include paranoid and persecutory delusions as well as auditory and visual hallucinations in the presence of extreme agitation. More common (about 18%) is for frequent amphetamine users to report psychotic symptoms that are sub-clinical and that do not require high-intensity intervention ...
About 5–15% of the users who develop an amphetamine psychosis fail to recover completely (Hofmann 1983) ...
Findings from one trial indicate use of antipsychotic medications effectively resolves symptoms of acute amphetamine psychosis.
psychotic symptoms of individuals with amphetamine psychosis may be due exclusively to heavy use of the drug or heavy use of the drug may exacerbate an underlying vulnerability to schizophrenia. - ^ Hofmann FG (1983). A Handbook on Drug and Alcohol Abuse: The Biomedical Aspects (ấn bản 2). New York, USA: Oxford University Press. tr. 329. ISBN 9780195030570.
- ^ Scassellati C, Bonvicini C, Faraone SV, Gennarelli M (tháng 10 năm 2012). “Biomarkers and attention-deficit/hyperactivity disorder: a systematic review and meta-analyses”. Journal of the American Academy of Child & Adolescent Psychiatry. 51 (10): 1003–1019.e20. doi:10.1016/j.jaac.2012.08.015. PMID 23021477.
With regard to zinc supplementation, a placebo controlled trial reported that doses up to 30 mg/day of zinc were safe for at least 8 weeks, but the clinical effect was equivocal except for the finding of a 37% reduction in amphetamine optimal dose with 30 mg per day of zinc.110
- ^ a b c d e f g h i j k l m n Eiden LE, Weihe E (tháng 1 năm 2011). “VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse”. Annals of the New York Academy of Sciences. 1216 (1): 86–98. doi:10.1111/j.1749-6632.2010.05906.x. PMC 4183197. PMID 21272013.
VMAT2 is the CNS vesicular transporter for not only the biogenic amines DA, NE, EPI, 5-HT, and HIS, but likely also for the trace amines TYR, PEA, and thyronamine (THYR) ... [Trace aminergic] neurons in mammalian CNS would be identifiable as neurons expressing VMAT2 for storage, and the biosynthetic enzyme aromatic amino acid decarboxylase (AADC). ... AMPH release of DA from synapses requires both an action at VMAT2 to release DA to the cytoplasm and a concerted release of DA from the cytoplasm via "reverse transport" through DAT.
- ^ a b c d e Sulzer D, Cragg SJ, Rice ME (tháng 8 năm 2016). “Striatal dopamine neurotransmission: regulation of release and uptake”. Basal Ganglia. 6 (3): 123–148. doi:10.1016/j.baga.2016.02.001. PMC 4850498. PMID 27141430.
Despite the challenges in determining synaptic vesicle pH, the proton gradient across the vesicle membrane is of fundamental importance for its function. Exposure of isolated catecholamine vesicles to protonophores collapses the pH gradient and rapidly redistributes transmitter from inside to outside the vesicle. ... Amphetamine and its derivatives like methamphetamine are weak base compounds that are the only widely used class of drugs known to elicit transmitter release by a non-exocytic mechanism. As substrates for both DAT and VMAT, amphetamines can be taken up to the cytosol and then sequestered in vesicles, where they act to collapse the vesicular pH gradient.
- ^ a b c Ledonne A, Berretta N, Davoli A, Rizzo GR, Bernardi G, Mercuri NB (tháng 7 năm 2011). “Electrophysiological effects of trace amines on mesencephalic dopaminergic neurons”. Frontiers in Systems Neuroscience. 5: 56. doi:10.3389/fnsys.2011.00056. PMC 3131148. PMID 21772817.
Three important new aspects of TAs action have recently emerged: (a) inhibition of firing due to increased release of dopamine; (b) reduction of D2 and GABAB receptor-mediated inhibitory responses (excitatory effects due to disinhibition); and (c) a direct TA1 receptor-mediated activation of GIRK channels which produce cell membrane hyperpolarization.
- ^ a b c “TAAR1”. GenAtlas. University of Paris. 28 tháng 1 năm 2012. Truy cập ngày 29 tháng 5 năm 2014.
• tonically activates inwardly rectifying K(+) channels, which reduces the basal firing frequency of dopamine (DA) neurons of the ventral tegmental area (VTA)
- ^ a b Lỗi chú thích: Thẻ
<ref>sai; không có nội dung trong thẻ ref có tênEAAT3 - ^ a b c Vaughan RA, Foster JD (tháng 9 năm 2013). “Mechanisms of dopamine transporter regulation in normal and disease states”. Trends in Pharmacological Sciences. 34 (9): 489–496. doi:10.1016/j.tips.2013.07.005. PMC 3831354. PMID 23968642.
AMPH and METH also stimulate DA efflux, which is thought to be a crucial element in their addictive properties [80], although the mechanisms do not appear to be identical for each drug [81]. These processes are PKCβ– and CaMK–dependent [72, 82], and PKCβ knock-out mice display decreased AMPH-induced efflux that correlates with reduced AMPH-induced locomotion [72].
- ^ a b “TA1 receptor”. IUPHAR database. International Union of Basic and Clinical Pharmacology. 2 tháng 12 năm 2014. Truy cập ngày 8 tháng 12 năm 2014.
- ^ Borowsky B, Adham N, Jones KA, Raddatz R, Artymyshyn R, Ogozalek KL, Durkin MM, Lakhlani PP, Bonini JA, Pathirana S, Boyle N, Pu X, Kouranova E, Lichtblau H, Ochoa FY, Branchek TA, Gerald C (tháng 7 năm 2001). “Trace amines: identification of a family of mammalian G protein-coupled receptors”. Proceedings of the National Academy of Sciences. 98 (16): 8966–8971. Bibcode:2001PNAS...98.8966B. doi:10.1073/pnas.151105198. PMC 55357. PMID 11459929.
- ^ a b Vicentic A, Jones DC (tháng 2 năm 2007). “The CART (cocaine- and amphetamine-regulated transcript) system in appetite and drug addiction”. Journal of Pharmacology and Experimental Therapeutics. 320 (2): 499–506. doi:10.1124/jpet.105.091512. PMID 16840648.
The physiological importance of CART was further substantiated in numerous human studies demonstrating a role of CART in both feeding and psychostimulant addiction. ... Colocalization studies also support a role for CART in the actions of psychostimulants. ... CART and DA receptor transcripts colocalize (Beaudry et al., 2004). Second, dopaminergic nerve terminals in the NAc synapse on CART-containing neurons (Koylu et al., 1999), hence providing the proximity required for neurotransmitter signaling. These studies suggest that DA plays a role in regulating CART gene expression possibly via the activation of CREB.
- ^ Zhang M, Han L, Xu Y (tháng 6 năm 2012). “Roles of cocaine- and amphetamine-regulated transcript in the central nervous system”. Clinical and Experimental Pharmacology and Physiology. 39 (6): 586–592. doi:10.1111/j.1440-1681.2011.05642.x. PMID 22077697.
Recently, it was demonstrated that CART, as a neurotrophic peptide, had a cerebroprotective against focal ischaemic stroke and inhibited the neurotoxicity of β-amyloid protein, which focused attention on the role of CART in the central nervous system (CNS) and neurological diseases. ... The literature indicates that there are many factors, such as regulation of the immunological system and protection against energy failure, that may be involved in the cerebroprotection afforded by CART
- ^ a b Rogge G, Jones D, Hubert GW, Lin Y, Kuhar MJ (tháng 10 năm 2008). “CART peptides: regulators of body weight, reward and other functions”. Nature Reviews Neuroscience. 9 (10): 747–758. doi:10.1038/nrn2493. PMC 4418456. PMID 18802445.
Several studies on CART (cocaine- and amphetamine-regulated transcript)-peptide-induced cell signalling have demonstrated that CART peptides activate at least three signalling mechanisms. First, CART 55–102 inhibited voltage-gated L-type Ca2+ channels ...
- ^ Lin Y, Hall RA, Kuhar MJ (tháng 10 năm 2011). “CART peptide stimulation of G protein-mediated signaling in differentiated PC12 cells: identification of PACAP 6–38 as a CART receptor antagonist”. Neuropeptides. 45 (5): 351–358. doi:10.1016/j.npep.2011.07.006. PMC 3170513. PMID 21855138.
- ^ Amphetamine. United States National Library of Medicine – National Center for Biotechnology Information. 11 tháng 4 năm 2015.
|ngày truy cập=cần|url=(trợ giúp) - ^ Monoamine oxidase (Homo sapiens). Technische Universität Braunschweig. 1 tháng 1 năm 2014. Truy cập ngày 4 tháng 5 năm 2014.
- ^ a b Amphetamine. University of Alberta. Truy cập ngày 24 tháng 2 năm 2015.
- ^ a b Toll L, Berzetei-Gurske IP, Polgar WE, Brandt SR, Adapa ID, Rodriguez L, Schwartz RW, Haggart D, O'Brien A, White A, Kennedy JM, Craymer K, Farrington L, Auh JS (tháng 3 năm 1998). “Standard binding and functional assays related to medications development division testing for potential cocaine and opiate narcotic treatment medications”. NIDA Research Monograph. 178: 440–466. PMID 9686407.
- ^ a b Finnema SJ, Scheinin M, Shahid M, Lehto J, Borroni E, Bang-Andersen B, Sallinen J, Wong E, Farde L, Halldin C, Grimwood S (tháng 11 năm 2015). “Application of cross-species PET imaging to assess neurotransmitter release in brain”. Psychopharmacology. 232 (21–22): 4129–4157. doi:10.1007/s00213-015-3938-6. PMC 4600473. PMID 25921033.
More recently, Colasanti and colleagues reported that a pharmacologically induced elevation in endogenous opioid release reduced [11C]carfentanil binding in several regions of the human brain, including the basal ganglia, frontal cortex, and thalamus (Colasanti et al. 2012). Oral administration of d-amphetamine, 0.5 mg/kg, 3 h before [11C]carfentanil injection, reduced BPND values by 2–10%. The results were confirmed in another group of subjects (Mick et al. 2014). However, Guterstam and colleagues observed no change in [11C]carfentanil binding when d-amphetamine, 0.3 mg/kg, was administered intravenously directly before injection of [11C]carfentanil (Guterstam et al. 2013). It has been hypothesized that this discrepancy may be related to delayed increases in extracellular opioid peptide concentrations following amphetamine-evoked monoamine release (Colasanti et al. 2012; Mick et al. 2014).
- ^ a b Loseth GE, Ellingsen DM, Leknes S (tháng 12 năm 2014). “State-dependent μ-opioid modulation of social motivation”. Frontiers in Behavioral Neuroscience. 8: 430. doi:10.3389/fnbeh.2014.00430. PMC 4264475. PMID 25565999.
Similar MOR activation patterns were reported during positive mood induced by an amusing video clip (Koepp et al., 2009) and following amphetamine administration in humans (Colasanti et al., 2012).
- ^ a b Colasanti A, Searle GE, Long CJ, Hill SP, Reiley RR, Quelch D, Erritzoe D, Tziortzi AC, Reed LJ, Lingford-Hughes AR, Waldman AD, Schruers KR, Matthews PM, Gunn RN, Nutt DJ, Rabiner EA (tháng 9 năm 2012). “Endogenous opioid release in the human brain reward system induced by acute amphetamine administration”. Biological Psychiatry. 72 (5): 371–377. doi:10.1016/j.biopsych.2012.01.027. PMID 22386378.
- ^ a b c Gunne LM (2013). “Effects of Amphetamines in Humans”. Drug Addiction II: Amphetamine, Psychotogen, and Marihuana Dependence. Berlin, Germany; Heidelberg, Germany: Springer. tr. 247–260. ISBN 9783642667091. Truy cập ngày 4 tháng 12 năm 2015.
- ^ a b c Oswald LM, Wong DF, McCaul M, Zhou Y, Kuwabara H, Choi L, Brasic J, Wand GS (tháng 4 năm 2005). “Relationships among ventral striatal dopamine release, cortisol secretion, and subjective responses to amphetamine”. Neuropsychopharmacology. 30 (4): 821–832. doi:10.1038/sj.npp.1300667. PMID 15702139.
Findings from several prior investigations have shown that plasma levels of glucocorticoids and ACTH are increased by acute administration of AMPH in both rodents and humans
- ^ a b Lewin AH, Miller GM, Gilmour B (tháng 12 năm 2011). “Trace amine-associated receptor 1 is a stereoselective binding site for compounds in the amphetamine class”. Bioorganic & Medicinal Chemistry. 19 (23): 7044–7048. doi:10.1016/j.bmc.2011.10.007. PMC 3236098. PMID 22037049.
- ^ a b Maguire JJ, Parker WA, Foord SM, Bonner TI, Neubig RR, Davenport AP (tháng 3 năm 2009). “International Union of Pharmacology. LXXII. Recommendations for trace amine receptor nomenclature”. Pharmacological Reviews. 61 (1): 1–8. doi:10.1124/pr.109.001107. PMC 2830119. PMID 19325074.
- ^ Revel FG, Moreau JL, Gainetdinov RR, Bradaia A, Sotnikova TD, Mory R, Durkin S, Zbinden KG, Norcross R, Meyer CA, Metzler V, Chaboz S, Ozmen L, Trube G, Pouzet B, Bettler B, Caron MG, Wettstein JG, Hoener MC (tháng 5 năm 2011). “TAAR1 activation modulates monoaminergic neurotransmission, preventing hyperdopaminergic and hypoglutamatergic activity”. Proceedings of the National Academy of Sciences. 108 (20): 8485–8490. doi:10.1073/pnas.1103029108. PMC 3101002. PMID 21525407.
- ^ a b Bozdag M, Altamimi AA, Vullo D, Supuran CT, Carta F (2019). “State of the Art on Carbonic Anhydrase Modulators for Biomedical Purposes”. Current Medicinal Chemistry. 26 (15): 2558–2573. doi:10.2174/0929867325666180622120625. PMID 29932025.
CARBONIC ANHYDRASE INHIBITORS (CAIs). The design and development of CAIs represent the most prolific area within the CA research field. Since the introduction of CAIs in the clinical use in the 40', they still are the first choice for the treatment of edema [9], altitude sickness [9], glaucoma [7] and epilepsy [31]. ... CARBONIC ANHYDRASE ACTIVATORS (CAAs) ... The emerging class of CAAs has recently gained attraction as the enhancement of the kinetic properties in hCAs expressed in the CNS were proved in animal models to be beneficial for the treatment of both cognitive and memory impairments. Thus, CAAs have enormous potentiality in medicinal chemistry to be developed for the treatment of symptoms associated to aging, trauma or deterioration of the CNS tissues.
- ^ a b c d e f g h i Ermer JC, Pennick M, Frick G (tháng 5 năm 2016). “Lisdexamfetamine Dimesylate: Prodrug Delivery, Amphetamine Exposure and Duration of Efficacy”. Clinical Drug Investigation. 36 (5): 341–356. doi:10.1007/s40261-015-0354-y. PMC 4823324. PMID 27021968.
- ^ a b c d e f “Vyvanse- lisdexamfetamine dimesylate capsule Vyvanse- lisdexamfetamine dimesylate tablet, chewable”. DailyMed. Shire US Inc. 30 tháng 10 năm 2019. Truy cập ngày 22 tháng 12 năm 2019. Lỗi chú thích: Thẻ
<ref>không hợp lệ: tên “USVyvanselabel” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ a b c d e Dolder PC, Strajhar P, Vizeli P, Hammann F, Odermatt A, Liechti ME (2017). “Pharmacokinetics and Pharmacodynamics of Lisdexamfetamine Compared with D-Amphetamine in Healthy Subjects”. Front Pharmacol. 8: 617. doi:10.3389/fphar.2017.00617. PMC 5594082. PMID 28936175.
Inactive lisdexamfetamine is completely (>98%) converted to its active metabolite D-amphetamine in the circulation (Pennick, 2010; Sharman and Pennick, 2014). When lisdexamfetamine is misused intranasally or intravenously, the pharmacokinetics are similar to oral use (Jasinski and Krishnan, 2009b; Ermer et al., 2011), and the subjective effects are not enhanced by parenteral administration in contrast to D-amphetamine (Lile et al., 2011) thus reducing the risk of parenteral misuse of lisdexamfetamine compared with D-amphetamine. Intravenous lisdexamfetamine use also produced significantly lower increases in "drug liking" and "stimulant effects" compared with D-amphetamine in intravenous substance users (Jasinski and Krishnan, 2009a).
- ^ p-Hydroxyamphetamine. United States National Library of Medicine – National Center for Biotechnology Information.
|ngày truy cập=cần|url=(trợ giúp) - ^ p-Hydroxynorephedrine. United States National Library of Medicine – National Center for Biotechnology Information.
|ngày truy cập=cần|url=(trợ giúp) - ^ Phenylpropanolamine. United States National Library of Medicine – National Center for Biotechnology Information.
|ngày truy cập=cần|url=(trợ giúp) - ^ Amphetamine. United States National Library of Medicine – National Center for Biotechnology Information.
|ngày truy cập=cần|url=(trợ giúp) - ^ a b c d e f Sjoerdsma A, von Studnitz W (tháng 4 năm 1963). “Dopamine-beta-oxidase activity in man, using hydroxyamphetamine as substrate”. British Journal of Pharmacology and Chemotherapy. 20: 278–284. doi:10.1111/j.1476-5381.1963.tb01467.x. PMC 1703637. PMID 13977820.
Hydroxyamphetamine was administered orally to five human subjects ... Since conversion of hydroxyamphetamine to hydroxynorephedrine occurs in vitro by the action of dopamine-β-oxidase, a simple method is suggested for measuring the activity of this enzyme and the effect of its inhibitors in man. ... The lack of effect of administration of neomycin to one patient indicates that the hydroxylation occurs in body tissues. ... a major portion of the β-hydroxylation of hydroxyamphetamine occurs in non-adrenal tissue. Unfortunately, at the present time one cannot be completely certain that the hydroxylation of hydroxyamphetamine in vivo is accomplished by the same enzyme which converts dopamine to noradrenaline.
- ^ a b c d Badenhorst CP, van der Sluis R, Erasmus E, van Dijk AA (tháng 9 năm 2013). “Glycine conjugation: importance in metabolism, the role of glycine N-acyltransferase, and factors that influence interindividual variation”. Expert Opinion on Drug Metabolism & Toxicology. 9 (9): 1139–1153. doi:10.1517/17425255.2013.796929. PMID 23650932.
Figure 1. Glycine conjugation of benzoic acid. The glycine conjugation pathway consists of two steps. First benzoate is ligated to CoASH to form the high-energy benzoyl-CoA thioester. This reaction is catalyzed by the HXM-A and HXM-B medium-chain acid:CoA ligases and requires energy in the form of ATP. ... The benzoyl-CoA is then conjugated to glycine by GLYAT to form hippuric acid, releasing CoASH. In addition to the factors listed in the boxes, the levels of ATP, CoASH, and glycine may influence the overall rate of the glycine conjugation pathway.
- ^ a b Horwitz D, Alexander RW, Lovenberg W, Keiser HR (tháng 5 năm 1973). “Human serum dopamine-β-hydroxylase. Relationship to hypertension and sympathetic activity”. Circulation Research. 32 (5): 594–599. doi:10.1161/01.RES.32.5.594. PMID 4713201.
The biologic significance of the different levels of serum DβH activity was studied in two ways. First, in vivo ability to β-hydroxylate the synthetic substrate hydroxyamphetamine was compared in two subjects with low serum DβH activity and two subjects with average activity. ... In one study, hydroxyamphetamine (Paredrine), a synthetic substrate for DβH, was administered to subjects with either low or average levels of serum DβH activity. The percent of the drug hydroxylated to hydroxynorephedrine was comparable in all subjects (6.5-9.62) (Table 3).
- ^ a b Freeman JJ, Sulser F (tháng 12 năm 1974). “Formation of p-hydroxynorephedrine in brain following intraventricular administration of p-hydroxyamphetamine”. Neuropharmacology. 13 (12): 1187–1190. doi:10.1016/0028-3908(74)90069-0. PMID 4457764.
In species where aromatic hydroxylation of amphetamine is the major metabolic pathway, p-hydroxyamphetamine (POH) and p-hydroxynorephedrine (PHN) may contribute to the pharmacological profile of the parent drug. ... The location of the p-hydroxylation and β-hydroxylation reactions is important in species where aromatic hydroxylation of amphetamine is the predominant pathway of metabolism. Following systemic administration of amphetamine to rats, POH has been found in urine and in plasma.
The observed lack of a significant accumulation of PHN in brain following the intraventricular administration of (+)-amphetamine and the formation of appreciable amounts of PHN from (+)-POH in brain tissue in vivo supports the view that the aromatic hydroxylation of amphetamine following its systemic administration occurs predominantly in the periphery, and that POH is then transported through the blood-brain barrier, taken up by noradrenergic neurones in brain where (+)-POH is converted in the storage vesicles by dopamine β-hydroxylase to PHN. - ^ a b Matsuda LA, Hanson GR, Gibb JW (tháng 12 năm 1989). “Neurochemical effects of amphetamine metabolites on central dopaminergic and serotonergic systems”. Journal of Pharmacology and Experimental Therapeutics. 251 (3): 901–908. PMID 2600821.
The metabolism of p-OHA to p-OHNor is well documented and dopamine-β hydroxylase present in noradrenergic neurons could easily convert p-OHA to p-OHNor after intraventricular administration.
- ^ a b c d ElRakaiby M, Dutilh BE, Rizkallah MR, Boleij A, Cole JN, Aziz RK (tháng 7 năm 2014). “Pharmacomicrobiomics: the impact of human microbiome variations on systems pharmacology and personalized therapeutics”. Omics. 18 (7): 402–414. doi:10.1089/omi.2014.0018. PMC 4086029. PMID 24785449.
The hundred trillion microbes and viruses residing in every human body, which outnumber human cells and contribute at least 100 times more genes than those encoded on the human genome (Ley et al., 2006), offer an immense accessory pool for inter-individual genetic variation that has been underestimated and largely unexplored (Savage, 1977; Medini et al., 2008; Minot et al., 2011; Wylie et al., 2012). ... Meanwhile, a wealth of literature has long been available about the biotransformation of xenobiotics, notably by gut bacteria (reviewed in Sousa et al., 2008; Rizkallah et al., 2010; Johnson et al., 2012; Haiser and Turnbaugh, 2013). This valuable information is predominantly about drug metabolism by unknown human-associated microbes; however, only a few cases of inter-individual microbiome variations have been documented [e.g., digoxin (Mathan et al., 1989) and acetaminophen (Clayton et al., 2009)].
- ^ a b Cho I, Blaser MJ (tháng 3 năm 2012). “The human microbiome: at the interface of health and disease”. Nature Reviews Genetics. 13 (4): 260–270. doi:10.1038/nrg3182. PMC 3418802. PMID 22411464.
The composition of the microbiome varies by anatomical site (Figure 1). The primary determinant of community composition is anatomical location: interpersonal variation is substantial23,24 and is higher than the temporal variability seen at most sites in a single individual25. ... How does the microbiome affect the pharmacology of medications? Can we "micro-type" people to improve pharmacokinetics and/or reduce toxicity? Can we manipulate the microbiome to improve pharmacokinetic stability?
- ^ Hutter T, Gimbert C, Bouchard F, Lapointe FJ (2015). “Being human is a gut feeling”. Microbiome. 3: 9. doi:10.1186/s40168-015-0076-7. PMC 4359430. PMID 25774294.
Some metagenomic studies have suggested that less than 10% of the cells that comprise our bodies are Homo sapiens cells. The remaining 90% are bacterial cells. The description of this so-called human microbiome is of great interest and importance for several reasons. For one, it helps us redefine what a biological individual is. We suggest that a human individual is now best described as a super-individual in which a large number of different species (including Homo sapiens) coexist.
- ^ a b c d Kumar K, Dhoke GV, Sharma AK, Jaiswal SK, Sharma VK (tháng 1 năm 2019). “Mechanistic elucidation of amphetamine metabolism by tyramine oxidase from human gut microbiota using molecular dynamics simulations”. Journal of Cellular Biochemistry. 120 (7): 11206–11215. doi:10.1002/jcb.28396. PMID 30701587.
Particularly in the case of the human gut, which harbors a large diversity of bacterial species, the differences in microbial composition can significantly alter the metabolic activity in the gut lumen.4 The differential metabolic activity due to the differences in gut microbial species has been recently linked with various metabolic disorders and diseases.5–12 In addition to the impact of gut microbial diversity or dysbiosis in various human diseases, there is an increasing amount of evidence which shows that the gut microbes can affect the bioavailability and efficacy of various orally administrated drug molecules through promiscuous enzymatic metabolism.13,14 ... The present study on the atomistic details of amphetamine binding and binding affinity to the tyramine oxidase along with the comparison with two natural substrates of this enzyme namely tyramine and phenylalanine provides strong evidence for the promiscuity-based metabolism of amphetamine by the tyramine oxidase enzyme of E. coli. The obtained results will be crucial in designing a surrogate molecule for amphetamine that can help either in improving the efficacy and bioavailability of the amphetamine drug via competitive inhibition or in redesigning the drug for better pharmacological effects. This study will also have useful clinical implications in reducing the gut microbiota caused variation in the drug response among different populations.
Lỗi chú thích: Thẻ<ref>không hợp lệ: tên “Microbial amphetamine metabolism - E. coli” được định rõ nhiều lần, mỗi lần có nội dung khác - ^ Thuật ngữ lấy từ [https://www.slideshare.net/hatoc5/chuyen-hoa-xenobiotic]
- ^ a b Khan MZ, Nawaz W (tháng 10 năm 2016). “The emerging roles of human trace amines and human trace amine-associated receptors (hTAARs) in central nervous system”. Biomedicine & Pharmacotherapy. 83: 439–449. doi:10.1016/j.biopha.2016.07.002. PMID 27424325.
- ^ a b c d e Lindemann L, Hoener MC (tháng 5 năm 2005). “A renaissance in trace amines inspired by a novel GPCR family”. Trends in Pharmacological Sciences. 26 (5): 274–281. doi:10.1016/j.tips.2005.03.007. PMID 15860375.
- ^ “Determination That Delcobese (Amphetamine Adipate, Amphetamine Sulfate, Dextroamphetamine Adipate, Dextroamphetamine Sulfate) Tablets and Capsules Were Not Withdrawn From Sale for Reasons of Safety or Effectiveness”. Federal Register. 10 tháng 11 năm 2003. Truy cập ngày 3 tháng 1 năm 2020.
- ^ Amphetamine Hydrochloride. United States National Library of Medicine – National Center for Biotechnology Information. Truy cập ngày 8 tháng 11 năm 2013.
- ^ Amphetamine Phosphate. United States National Library of Medicine – National Center for Biotechnology Information. Truy cập ngày 8 tháng 11 năm 2013.
- ^ Cavallito, John (23 tháng 8 năm 1960). “Amphetamine Tannate. Patent Application No. 2,950,309” (PDF). United States Patent Office. Lưu trữ (PDF) bản gốc ngày 9 tháng 10 năm 2022.
- ^ Brussee J, Jansen AC (tháng 5 năm 1983). “A highly stereoselective synthesis of s(−)-[1,1'-binaphthalene]-2,2'-diol”. Tetrahedron Letters. 24 (31): 3261–3262. doi:10.1016/S0040-4039(00)88151-4.
- ^ a b Hagel JM, Krizevski R, Marsolais F, Lewinsohn E, Facchini PJ (2012). “Biosynthesis of amphetamine analogs in plants”. Trends in Plant Science. 17 (7): 404–412. doi:10.1016/j.tplants.2012.03.004. PMID 22502775.
Substituted amphetamines, which are also called phenylpropylamino alkaloids, are a diverse group of nitrogen-containing compounds that feature a phenethylamine backbone with a methyl group at the α-position relative to the nitrogen (Figure 1). ... Beyond (1R,2S)-ephedrine and (1S,2S)-pseudoephedrine, myriad other substituted amphetamines have important pharmaceutical applications. ... For example, (S)-amphetamine (Figure 4b), a key ingredient in Adderall and Dexedrine, is used to treat attention deficit hyperactivity disorder (ADHD) [79]. ...
[Figure 4](b) Examples of synthetic, pharmaceutically important substituted amphetamines. - ^ a b Schep LJ, Slaughter RJ, Beasley DM (tháng 8 năm 2010). “The clinical toxicology of metamfetamine”. Clinical Toxicology. 48 (7): 675–694. doi:10.3109/15563650.2010.516752. ISSN 1556-3650. PMID 20849327.
- ^ Lillsunde P, Korte T (tháng 3 năm 1991). “Determination of ring- and N-substituted amphetamines as heptafluorobutyryl derivatives”. Forensic Science International. 49 (2): 205–213. doi:10.1016/0379-0738(91)90081-s. PMID 1855720.
- ^ a b c d “Historical overview of methamphetamine”. Vermont Department of Health. Government of Vermont. Bản gốc lưu trữ ngày 5 tháng 10 năm 2012. Truy cập ngày 29 tháng 1 năm 2012.
- ^ a b c Allen A, Ely R (tháng 4 năm 2009). “Review: Synthetic Methods for Amphetamine” (PDF). Crime Scene. Northwest Association of Forensic Scientists. 37 (2): 15–25. Truy cập ngày 6 tháng 12 năm 2014.
- ^ a b c Allen A, Cantrell TS (tháng 8 năm 1989). “Synthetic reductions in clandestine amphetamine and methamphetamine laboratories: A review”. Forensic Science International. 42 (3): 183–199. doi:10.1016/0379-0738(89)90086-8.
- ^ a b c d “Recommended methods of the identification and analysis of amphetamine, methamphetamine, and their ring-substituted analogues in seized materials” (PDF). United Nations Office on Drugs and Crime. United Nations. 2006. tr. 9–12. Truy cập ngày 14 tháng 10 năm 2013.
- ^ Pollard CB, Young DC (tháng 5 năm 1951). “The Mechanism of the Leuckart Reaction”. The Journal of Organic Chemistry. 16 (5): 661–672. doi:10.1021/jo01145a001.
- ^ a b Gray DL (2007). “Approved Treatments for Attention Deficit Hyperactivity Disorder: Amphetamine (Adderall), Methylphenidate (Ritalin), and Atomoxetine (Straterra)”. Trong Johnson DS, Li JJ (biên tập). The Art of Drug Synthesis. New York, USA: Wiley-Interscience. tr. 247. ISBN 9780471752158.
- ^ Patrick TM, McBee ET, Hass HB (tháng 6 năm 1946). “Synthesis of arylpropylamines; from allyl chloride”. Journal of the American Chemical Society. 68 (6): 1009–1011. doi:10.1021/ja01210a032. PMID 20985610.
- ^ Ritter JJ, Kalish J (tháng 12 năm 1948). “A new reaction of nitriles; synthesis of t-carbinamines”. Journal of the American Chemical Society. 70 (12): 4048–4050. doi:10.1021/ja01192a023. PMID 18105933.
- ^ Krimen LI, Cota DJ (tháng 3 năm 2011). “The Ritter Reaction”. Organic Reactions. 17. tr. 216. doi:10.1002/0471264180.or017.03. ISBN 9780471264187.
- ^ Collins M, Salouros H, Cawley AT, Robertson J, Heagney AC, Arenas-Queralt A (tháng 6 năm 2010). “δ13C and δ2H isotope ratios in amphetamine synthesized from benzaldehyde and nitroethane”. Rapid Communications in Mass Spectrometry. 24 (11): 1653–1658. doi:10.1002/rcm.4563. PMID 20486262.
- ^ a b “Clinical Drug Testing in Primary Care” (PDF). University of Colorado Denver. Technical Assistance Publication Series 32. United States Department of Health and Human Services – Substance Abuse and Mental Health Services Administration. 2012. tr. 55. Lưu trữ (PDF) bản gốc ngày 14 tháng 5 năm 2018. Truy cập ngày 31 tháng 10 năm 2013.
A single dose of amphetamine or methamphetamine can be detected in the urine for approximately 24 hours, depending upon urine pH and individual metabolic differences. People who use chronically and at high doses may continue to have positive urine specimens for 2–4 days after last use (SAMHSA, 2010b).
- ^ a b c d e Paul BD, Jemionek J, Lesser D, Jacobs A, Searles DA (tháng 9 năm 2004). “Enantiomeric separation and quantitation of (±)-amphetamine, (±)-methamphetamine, (±)-MDA, (±)-MDMA, and (±)-MDEA in urine specimens by GC-EI-MS after derivatization with (R)-(−)- or (S)-(+)-α-methoxy-α-(trifluoromethyl)phenylacetyl chloride (MTPA)”. Journal of Analytical Toxicology. 28 (6): 449–455. doi:10.1093/jat/28.6.449. PMID 15516295.
- ^ a b Verstraete AG, Heyden FV (tháng 8 năm 2005). “Comparison of the sensitivity and specificity of six immunoassays for the detection of amphetamines in urine”. Journal of Analytical Toxicology. 29 (5): 359–364. doi:10.1093/jat/29.5.359. PMID 16105261.
- ^ Baselt RC (2011). Disposition of Toxic Drugs and Chemicals in Man (ấn bản 9). Seal Beach, USA: Biomedical Publications. tr. 85–88. ISBN 9780962652387.
- ^ a b Musshoff F (tháng 2 năm 2000). “Illegal or legitimate use? Precursor compounds to amphetamine and methamphetamine”. Drug Metabolism Reviews. 32 (1): 15–44. doi:10.1081/DMR-100100562. PMID 10711406.
- ^ a b Cody JT (tháng 5 năm 2002). “Precursor medications as a source of methamphetamine and/or amphetamine positive drug testing results”. Journal of Occupational and Environmental Medicine. 44 (5): 435–450. doi:10.1097/00043764-200205000-00012. PMID 12024689.
- ^ “WDR 2022_Booklet 1”. United Nations : Office on Drugs and Crime (bằng tiếng Anh). Truy cập ngày 29 tháng 10 năm 2022.
- ^ Bản pdf (PDF). tr. 60.
- ^ a b c Morelli M, Tognotti E (tháng 8 năm 2021). “Brief history of the medical and non-medical use of amphetamine-like psychostimulants”. Exp Neurol. 342: 113754. doi:10.1016/j.expneurol.2021.113754. PMID 34000249.
- ^ Wood S, Sage JR, Shuman T, Anagnostaras SG (2014). “Psychostimulants and cognition: a continuum of behavioral and cognitive activation”. Pharmacol Rev. 66 (1): 193–221. doi:10.1124/pr.112.007054. PMC 3880463. PMID 24344115.
- ^ Rassool GH (2009). Alcohol and Drug Misuse: A Handbook for Students and Health Professionals. London, England: Routledge. tr. 113. ISBN 9780203871171.
- ^ a b Sulzer D, Sonders MS, Poulsen NW, Galli A (tháng 4 năm 2005). “Mechanisms of neurotransmitter release by amphetamines: a review”. Progress in Neurobiology. 75 (6): 406–433. doi:10.1016/j.pneurobio.2005.04.003. PMID 15955613.
- ^ Rasmussen N (tháng 8 năm 2011). “Medical science and the military: the Allies' use of amphetamine during World War II”. Journal of Interdisciplinary History. 42 (2): 205–233. doi:10.1162/JINH_a_00212. PMID 22073434.
- ^ Defalque RJ, Wright AJ (tháng 4 năm 2011). “Methamphetamine for Hitler's Germany: 1937 to 1945”. Bulletin of Anesthesia History. 29 (2): 21–24, 32. doi:10.1016/s1522-8649(11)50016-2. PMID 22849208.
- ^ “Controlled Substances Act”. United States Food and Drug Administration. 11 tháng 6 năm 2009. Bản gốc lưu trữ ngày 2 tháng 3 năm 2017. Truy cập ngày 4 tháng 11 năm 2013.
- ^ “Controlled Substance Schedules”. DEA Diversion Control Division. Truy cập ngày 25 tháng 12 năm 2019.
- ^ Gyenis A. “Forty Years of On the Road 1957–1997”. wordsareimportant.com. DHARMA beat. Bản gốc lưu trữ ngày 14 tháng 2 năm 2008. Truy cập ngày 18 tháng 3 năm 2008.
- ^ Wilson A (2008). “Mixing the Medicine: The unintended consequence of amphetamine control on the Northern Soul Scene” (PDF). Internet Journal of Criminology. Bản gốc (PDF) lưu trữ ngày 13 tháng 7 năm 2011. Truy cập ngày 25 tháng 5 năm 2013.
- ^ Hill J (4 tháng 6 năm 2004). “Paul Erdos, Mathematical Genius, Human (In That Order)” (PDF). Truy cập ngày 2 tháng 11 năm 2013.
- ^ a b c Mohan J biên tập (tháng 6 năm 2014). “World Drug Report 2014” (PDF). United Nations Office on Drugs and Crime. tr. 3. Truy cập ngày 18 tháng 8 năm 2014.
- ^ “Statistical Bulletin 2018 − prevalence of drug use”. European Monitoring Centre for Drugs and Drug Addiction. Truy cập ngày 5 tháng 2 năm 2019.
- ^ a b European Monitoring Centre for Drugs Drug Addiction (tháng 5 năm 2014). European drug report 2014: Trends and developments (PDF) (Bản báo cáo). Lisbon, Portugal: European Monitoring Centre for Drugs and Drug Addiction. tr. 13, 24. doi:10.2810/32306. ISSN 2314-9086. Bản gốc (PDF) lưu trữ ngày 9 tháng 10 năm 2022. Truy cập ngày 18 tháng 8 năm 2014.
1.2 million or 0.9% of young adults (15–34) used amphetamines in the last year
- ^ United Nations Office on Drugs and Crime (2007). Preventing Amphetamine-type Stimulant Use Among Young People: A Policy and Programming Guide (PDF). New York, USA: United Nations. ISBN 9789211482232. Truy cập ngày 11 tháng 11 năm 2013.
- ^ “List of psychotropic substances under international control” (PDF). International Narcotics Control Board. United Nations. tháng 8 năm 2003. Bản gốc (PDF) lưu trữ ngày 5 tháng 12 năm 2005. Truy cập ngày 19 tháng 11 năm 2005.
- ^ “Importing or Bringing Medication into Japan for Personal Use”. Japanese Ministry of Health, Labour and Welfare. 1 tháng 4 năm 2004. Truy cập ngày 3 tháng 11 năm 2013.
- ^ “Controlled Drugs and Substances Act”. Canadian Justice Laws Website. Government of Canada. Bản gốc lưu trữ ngày 22 tháng 11 năm 2013. Truy cập ngày 11 tháng 11 năm 2013.
- ^ “Opiumwet”. Government of the Netherlands. Truy cập ngày 3 tháng 4 năm 2015.
- ^ Poisons Standard. Australian Government Department of Health. tháng 10 năm 2015. Truy cập ngày 15 tháng 12 năm 2015.
- ^ “Table of controlled Narcotic Drugs under the Thai Narcotics Act” (PDF). Thailand Food and Drug Administration. 22 tháng 5 năm 2013. Bản gốc (PDF) lưu trữ ngày 8 tháng 3 năm 2014. Truy cập ngày 11 tháng 11 năm 2013.
- ^ “Class A, B and C drugs”. Home Office, Government of the United Kingdom. Bản gốc lưu trữ ngày 4 tháng 8 năm 2007. Truy cập ngày 23 tháng 7 năm 2007.
- ^ a b “Adzenys XR-ODT- amphetamine tablet, orally disintegrating”. DailyMed. Neos Therapeutics, Inc. 9 tháng 2 năm 2018. Truy cập ngày 22 tháng 12 năm 2019.
ADZENYS XR-ODT (amphetamine extended-release orally disintegrating tablet) contains a 3 to 1 ratio of d- to l-amphetamine, a central nervous system stimulant.
- ^ “Mydayis- dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate capsule, extended release”. DailyMed. Shire US Inc. 11 tháng 10 năm 2019. Truy cập ngày 22 tháng 12 năm 2019.
- ^ “Drug Approval Package: Mydayis (mixed salts of a single-entity amphetamine product)”. United States Food and Drug Administration. 6 tháng 6 năm 2018. Truy cập ngày 22 tháng 12 năm 2019.
- ^ “Adzenys ER- amphetamine suspension, extended release”. DailyMed. Neos Therapeutics, Inc. 8 tháng 12 năm 2017. Truy cập ngày 25 tháng 12 năm 2019.
- ^ “Drug Approval Package: Adzenys XR-ODT (amphetamine)”. United States Food and Drug Administration. Truy cập ngày 22 tháng 12 năm 2019.
- ^ “Evekeo”. United States Food and Drug Administration. Truy cập ngày 11 tháng 8 năm 2015.
- ^ “Evekeo ODT- amphetamine sulfate tablet, orally disintegrating”. DailyMed. Arbor Pharmaceuticals, LLC. 7 tháng 6 năm 2019. Truy cập ngày 25 tháng 12 năm 2019.
- ^ “Zenzedi- dextroamphetamine sulfate tablet”. DailyMed. Arbor Pharmaceuticals, LLC. 14 tháng 8 năm 2019. Truy cập ngày 22 tháng 12 năm 2019.
- ^ “Drug Approval Package: Vyvanse (Lisdexamfetamine Dimesylate) NDA #021977”. United States Food and Drug Administration. 24 tháng 12 năm 1999. Truy cập ngày 22 tháng 12 năm 2019.
- ^ “Approval [Rx ONLY]” (PDF). U.S. Food and Drug Administration. Truy cập ngày 11 tháng 10 năm 2022.
Lỗi chú thích: Đã tìm thấy thẻ <ref> với tên nhóm “note”, nhưng không tìm thấy thẻ tương ứng <references group="note"/> tương ứng, hoặc thẻ đóng </ref> bị thiếu
Lỗi chú thích: Đã tìm thấy thẻ <ref> với tên nhóm “sources”, nhưng không tìm thấy thẻ tương ứng <references group="sources"/> tương ứng, hoặc thẻ đóng </ref> bị thiếu
Lỗi chú thích: Đã tìm thấy thẻ <ref> với tên nhóm “Chú thích màu sắc”, nhưng không tìm thấy thẻ tương ứng <references group="Chú thích màu sắc"/> tương ứng, hoặc thẻ đóng </ref> bị thiếu
Lỗi chú thích: Đã tìm thấy thẻ <ref> với tên nhóm “cụm nguồn”, nhưng không tìm thấy thẻ tương ứng <references group="cụm nguồn"/> tương ứng, hoặc thẻ đóng </ref> bị thiếu
Lỗi chú thích: Đã tìm thấy thẻ <ref> với tên nhóm “chú thích”, nhưng không tìm thấy thẻ tương ứng <references group="chú thích"/> tương ứng, hoặc thẻ đóng </ref> bị thiếu